Nursing Technology and workflow efficiency: Discover how nurses can integrate Smart Devices in Nursing Workflow without increasing burnout. Expert insights from a Ghanaian RN with 10+ years of experience.
Table of Contents
Introduction: The Double-Edged Promise of Smart Technology in Nursing
There is a moment every nurse knows — standing at a bedside at 2 AM, juggling four IV lines, a restless post-operative patient, and an alarm sounding from down the hall, all while trying to document in an electronic health record that is loading slower than acceptable. Your feet ache. Your mind is racing. And somewhere in the back of your head, you are wondering: Was this supposed to get easier with technology?
I am Abdul-Muumin Wedraogo, a Registered General Nurse with over ten years of frontline experience across Emergency, ICU, Pediatrics, and General Ward settings under the Ghana Health Service. I also hold a Diploma in Network Engineering and an Advanced Professional certification in System Engineering, which means I sit at a unique intersection: I understand nursing workflows from the bedside and the systems that support them from the backend.
And I can tell you plainly: smart devices in nursing are not inherently a burden. But they can become one if introduced carelessly.
According to the World Health Organization (2023), nurse burnout is now recognized as a global occupational phenomenon threatening healthcare quality and workforce sustainability across high-, middle-, and low-income countries alike. In Sub-Saharan Africa, where nurse-to-patient ratios routinely exceed international recommendations, this crisis is especially acute (WHO, 2023).
At the same time, the global smart healthcare device market is projected to surpass $167 billion by 2030 (Grand View Research, 2023). Wearables, mobile clinical apps, AI-assisted monitoring, smart infusion pumps, and point-of-care diagnostic devices are flooding hospital environments — promising efficiency gains that sometimes fail to materialize when implementation is poor.
In this article, you will learn:
- Which smart devices genuinely improve nursing workflow versus those that add complexity
- How to integrate technology into clinical practice without increasing cognitive overload
- The cybersecurity and ethical considerations every nurse must understand
- How African hospitals can adapt global innovations to local realities
- Practical, step-by-step strategies for sustainable technology adoption
This is not a tech sales pitch. This is a clinically grounded, evidence-based guide written from the ward floor up.

Real-World Clinical Context: Technology at 3 AM in the Emergency Department
Let me paint a picture from my own experience.
It was a night shift in the emergency department. We had a surge — twelve patients waiting, three in active resuscitation bays, and staffing was stretched thin as it so often is in Ghanaian public hospitals. A young man in Bay 2 had sepsis, his blood pressure trending downward, and I was managing his fluid resuscitation while simultaneously monitoring a pediatric patient with severe malaria across the room.
At that moment, a traditional pulse oximeter alarm went off in Bay 3 — a false alarm triggered by patient movement. I had to physically walk over, silence it, reassess the patient, and document the interruption. That took four minutes.
Four minutes in a resuscitation environment is not trivial.
Now contrast that scenario with what a hospital equipped with smart monitoring devices would look like: continuous wireless telemetry sending data directly to a central nursing dashboard and to my clinical smartwatch. The false alarm would be filtered by AI pattern recognition. The alert reaching me would be intelligent — context-sensitive, prioritized, and actionable.
That is the promise of smart nursing technology. But here is the critical insight most technology vendors will not tell you: the problem is never just the device. The problem is integration — how the device fits into the cognitive and physical flow of a nurse’s shift.

Understanding Nursing Workflow: Before You Add a Device, Understand the Flow
What Is a Nursing Workflow?
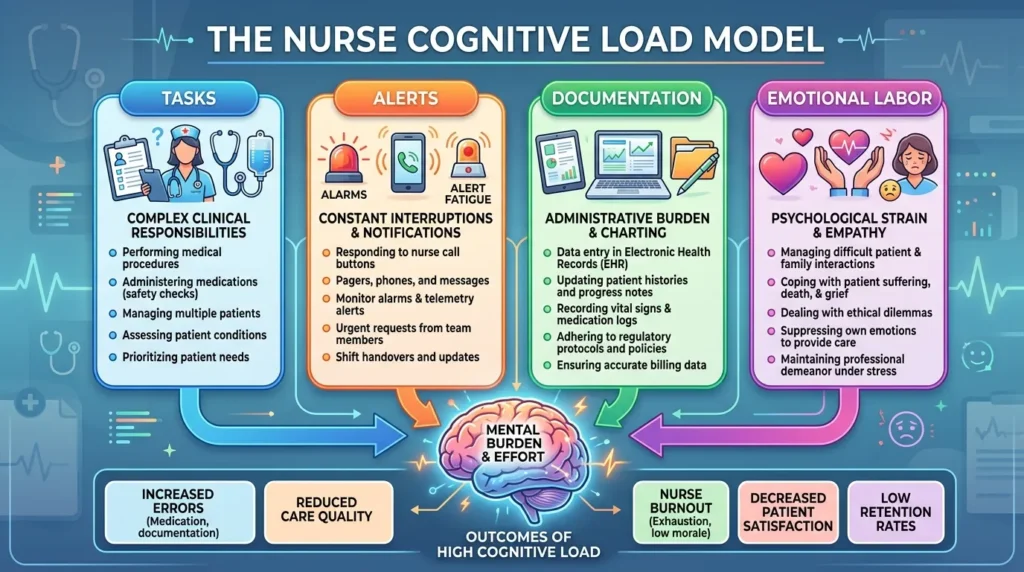
A nursing workflow is not simply a task list. It is a dynamic, adaptive cognitive process — one where a nurse is simultaneously prioritizing, communicating, assessing, documenting, and responding to changes in real time. Registered nurses operating in high-acuity environments can manage up to 12–15 distinct cognitive tasks within a single hour (Cornell et al., 2011).
Nursing workflows are characterized by:
- Frequent interruptions (average of 6.7 interruptions per hour in clinical settings)
- High cognitive load (medication calculations, differential assessment, patient education)
- Physical demands (patient mobilization, equipment handling, shift-long standing)
- Emotional labor (family communication, end-of-life care, trauma exposure)
Adding a new smart device into this environment without careful planning does not reduce burden — it adds a new cognitive layer that must be managed alongside everything else.
The Cognitive Load Problem
Cognitive load theory, developed by Sweller (1988) and widely applied in healthcare education, describes how human working memory has a finite capacity. When nurses are overloaded cognitively — managing too many simultaneous tasks or alerts — errors increase, and performance degrades (Hicks et al., 2015).
Many smart devices, particularly those that generate high volumes of alerts, worsen cognitive overload rather than relieve it. This is called alert fatigue — a documented phenomenon where nurses become desensitized to device alarms because so many are false positives (Drew et al., 2014).
The solution is not to reject technology. It is to select and implement technology that genuinely reduces cognitive load by making information more accessible, more contextual, and more actionable — without demanding additional attention.
Types of Smart Devices in Nursing Workflow
1. Wearable Vital Signs Monitors
Wearable patient monitors — devices like continuous SpO2 patches, wireless ECG monitors, and non-invasive blood pressure cuffs — are among the most impactful technologies for nursing workflow when implemented correctly.
How they help:
- Eliminate the need for manual vital sign rounds every 2–4 hours
- Provide continuous data streams that catch deterioration earlier
- Free nursing time for higher-level care tasks (assessment, education, emotional support)
- Reduce the physical burden of dragging traditional monitoring equipment from room to room
Clinical evidence: A 2019 study published in the Journal of Nursing Management found that implementing continuous wireless patient monitoring reduced nurse response time to clinical deterioration by 38% while simultaneously decreasing the number of physical patient checks by nursing staff (Downey et al., 2019).
African context: Devices like the Masimo Radius PPG and Biobeat continuous monitoring patches have been trialed in several African hospital environments. Cost remains a barrier, but shared-device models — where a small fleet of monitors rotates across high-risk patients — are a feasible middle ground for resource-limited settings.

2. Clinical Smartwatches and Wearables for Nurses
Smartwatches designed specifically for clinical environments — such as the Apple Watch (with clinical-grade apps), Samsung Galaxy Watch, and purpose-built devices like the Garmin vívoactive — serve a different function than patient monitoring. These devices support the nurse’s own physiological and operational well-being.
Nursing-relevant features:
- Pulse and HRV monitoring (tracking personal stress and fatigue levels)
- Quiet haptic alerts for medication reminders and patient alerts
- Step and posture tracking over long shifts
- Integrated clinical reference apps (drug dosing, clinical calculators)
- Hands-free timer functions for medication administration timing
Why this matters for burnout: A 2022 systematic review in Worldviews on Evidence-Based Nursing found that wearable wellness devices, when combined with institutional wellness programs, significantly reduced self-reported burnout scores among ICU nurses over 6 months (Labrague et al., 2022).
The keyword is “combined.” A smartwatch alone does not reduce burnout. But a smartwatch worn by a nurse who is supported by a hospital that actually monitors and responds to wellbeing data — that creates change.
Practical note for Ghanaian nurses: Many clinical-grade smartwatch features are accessible on mid-range devices at GHS 600–1200. Nurses do not need premium hardware to benefit from quiet alert routing, step tracking, and reference applications.

3. Mobile Clinical Apps
Smartphones are already present in most nursing environments — often unofficially. Rather than fighting this reality, forward-thinking hospitals are formalizing mobile clinical app adoption within structured frameworks.
High-value nursing apps include:
| Category | App Examples | Function |
| Drug reference | Epocrates, Medscape | Medication checking, interactions |
| Clinical calculators | MedCalc, Calculate by QxMD | Dosing, risk scores |
| Shift scheduling | NurseGrid, ShiftKey | Schedule management |
| Communication | Vocera, TigerConnect | Secure clinical messaging |
| Mental health | Calm, Headspace for Work | Nurse wellness |
| EHR mobile access | Epic Haiku, Cerner PowerChart | Documentation on the go |
Alert fatigue management: The most dangerous aspect of mobile clinical apps is unrestricted notification overload. Nurses using five or more apps without notification management protocols report higher rates of distraction errors (Keller et al., 2020). Hospitals must implement notification governance — defining which alerts warrant immediate interruption versus passive review.

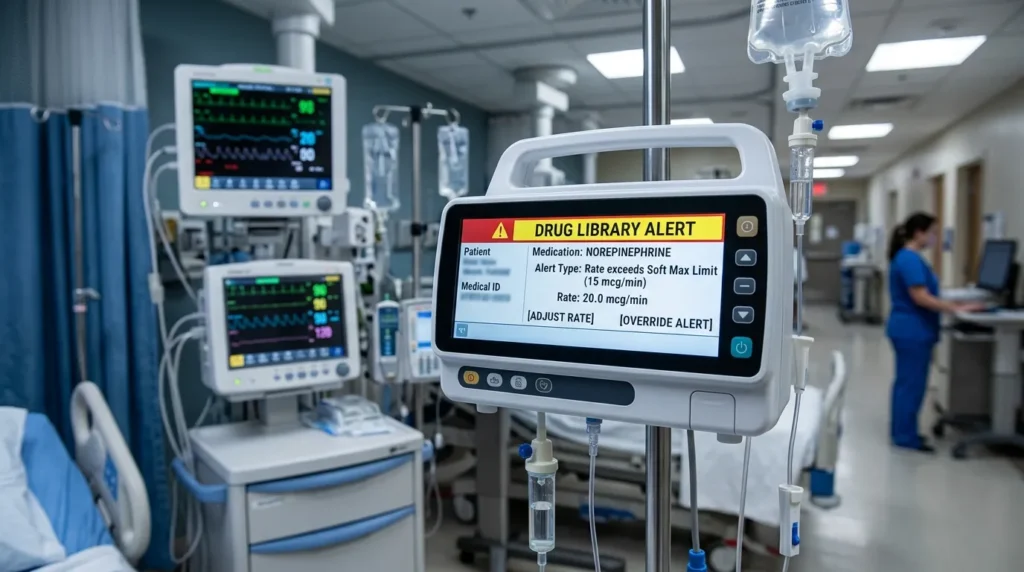
4. Smart Infusion Pumps
Smart infusion pumps with dose-error reduction software (DERS) represent one of the most evidence-supported technology investments in nursing care. The Institute for Safe Medication Practices (ISMP) and major nursing organizations have long advocated for their adoption.
Key benefits:
- Drug library integration prevents common dosing errors
- Alerts for rate changes outside safe parameters
- Automatic documentation of infusion data to EHR
- Reduction in “free-flow” incidents that historically caused patient harm
Evidence: A landmark study by Nuckols et al. (2016) found that smart pump adoption with DERS was associated with a 50–80% reduction in serious medication error rates in ICU settings. Critically, nursing workload decreased with smart pumps because nurses spent less time recalculating rates and managing secondary checks.
For African hospitals: Smart infusion pumps remain financially prohibitive for many public sector facilities in Ghana and across Sub-Saharan Africa. However, GHS procurement partnerships and donor-supported pilot programs (e.g., through global health initiatives) represent pathways to access.
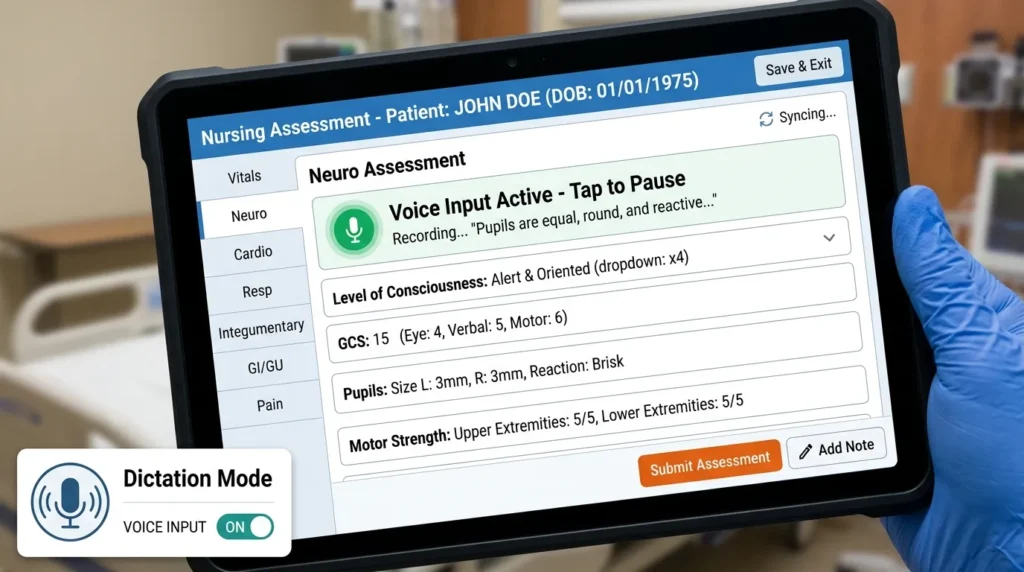
5. Electronic Health Records (EHR) and Bedside Tablets
EHR systems, when poorly designed and implemented, are among the leading contributors to nurse burnout. However, when designed with nursing workflow in mind and accessed via bedside tablets, they can genuinely streamline documentation.
Workflow-positive EHR features:
- Voice-to-text documentation (reduces typing burden)
- Pre-populated assessment templates
- Real-time order visibility
- Integrated clinical decision support
The burnout risk: Studies consistently show that EHR systems designed primarily around physician workflows — with nursing documentation as an afterthought — increase nurse cognitive burden (Poissant et al., 2005). The solution is nurse involvement in EHR design and procurement decisions. Nurses must have a seat at the technology table.
Comparison Table: Smart Devices for Nursing Workflow
| Feature | Wearable Patient Monitor | Clinical Smartwatch (Nurse) | Smart Infusion Pump | Mobile Clinical App |
| Primary Benefit | Continuous patient monitoring | Nurse wellness + alerts | Medication safety | Clinical reference + communication |
| Burnout Impact | Reduces if alerts are managed | Reduces with wellness features | Reduces medication anxiety | Mixed (depends on notification management) |
| Cost Range | High ($500–$5000/device) | Low–Medium ($200–$800) | High ($3000–$8000) | Low–Free ($0–$50/month) |
| HIPAA/Data Compliance | Requires a secure network | Depends on the apps used | Built-in compliance | Varies by app |
| Ease of Use | Moderate (training required) | High (intuitive) | Moderate (training required) | High |
| African Hospital Suitability | Challenging (cost) | High | Challenging (cost) | High |
| Best For | ICU, High Dependency Units | All nursing environments | ICU, oncology, perioperative | All nursing environments |
The Burnout Connection: Why Technology Can Make Things Worse
This cannot be glossed over. Technology can increase burnout, and understanding how is as important as understanding how it helps.
Alert Fatigue: The Silent Burnout Accelerator
Alert fatigue is defined as the desensitization of healthcare providers to safety alerts, resulting from exposure to an overwhelming number of alarms — many of which are false or clinically irrelevant (Drew et al., 2014).
Research from Johns Hopkins found that in a 15-bed cardiac ICU, monitors generated an average of 942 alarms per bed per day, of which more than 88% were clinically non-actionable (Cvach, 2012). Nurses operating in this environment experience chronic sympathetic nervous system activation — the physiological state of sustained stress.
Over time, this produces:
- Alarm desensitization (nurses begin ignoring alarms)
- Increased anxiety and hypervigilance during off-duty hours
- Sleep disruption between shifts
- Accelerated professional burnout
The solution is alarm management policy: hospitals must define alarm thresholds, implement individualized alarm parameters, use AI-driven alarm filtering, and audit alarm data regularly. This is a systems problem — not a nursing problem.
Technology Inequality and Frustration
In healthcare environments where some wards have advanced smart devices and others have none — or where devices are available but not maintained or updated — nurses in under-resourced areas experience technology frustration. This inequity, well-documented in Ghanaian and broader West African hospital settings, generates resentment and demoralizes staff who see the gap between available tools and what they need to deliver safe care (Agyemang-Duah et al., 2021).
Sustainable smart device implementation must include equity planning: what happens to the ward that does not receive the first round of devices? How are maintenance and repair funded? These are not peripheral questions — they are central to preventing technology from becoming a new axis of nursing burnout.
Cybersecurity and Ethical Considerations: What Every Nurse Must Know
Given my background in Network Engineering and System Engineering, this section is particularly close to my practice. The convergence of clinical devices and digital networks creates a security surface that most nurses are never trained to navigate — and that gap is dangerous.
The Cybersecurity Risk Landscape in Healthcare
Hospitals are among the most targeted sectors for cyberattacks globally. According to the IBM Security Cost of a Data Breach Report (2023), the average cost of a healthcare data breach reached $10.9 million — the highest of any industry for the thirteenth consecutive year.
Why nursing-related devices are targets:
- Smart devices connected to hospital networks are entry points for ransomware
- Patient data transmitted from wearables and monitoring devices is valuable on dark web markets
- Nurses using personal devices for clinical communication create shadow IT vulnerabilities
- Unsecured Wi-Fi access for smart device data transmission exposes protected health information (PHI)
HIPAA, GDPR, and Ghana Data Protection Principles
HIPAA (Health Insurance Portability and Accountability Act) applies to U.S. healthcare providers but is internationally recognized as the benchmark for patient data protection. Its principles — minimum necessary access, encryption of PHI in transit and at rest, audit trails — should guide smart device procurement anywhere.
GDPR (General Data Protection Regulation) applies to European patients and institutions but sets a global standard for how biometric and health data collected by wearable devices must be handled.
Ghana’s Data Protection Act (Act 843, 2012) governs personal data processing in Ghana, including health data. Nurses working with smart devices that collect patient data are legally obligated to ensure that data processing complies with Act 843 — yet very few Ghanaian nurses receive training on this obligation.
Safe Device Usage: A Practical Cybersecurity Guide for Nurses
- Never connect personal devices to hospital clinical networks without IT authorization.
- Use only hospital-approved apps for clinical communication — personal WhatsApp and standard SMS are not secure for patient information.
- Lock device screens between use — unattended unlocked tablets or phones in clinical areas are a breach risk.
- Report suspicious device behavior immediately — slow performance, unexpected restarts, or unfamiliar apps may indicate compromise.
- Attend annual cybersecurity training — this is as important as clinical skills updates.
- Challenge vendors on data practices — where is device data stored? Who has access? Is it encrypted? These are non-negotiable questions before adopting any smart device.
AI Ethics in Nursing: Bias, Accountability, and Transparency
Artificial intelligence is increasingly embedded in clinical smart devices — from predictive deterioration algorithms to AI-assisted diagnostic imaging. Nurses must understand the ethical dimensions:
AI bias: Many clinical AI algorithms were trained on datasets that underrepresent African and other non-Western patient populations, creating accuracy disparities. An AI sepsis prediction tool trained primarily on North American ICU data may perform differently in a Ghanaian hospital environment. Nurses must question — and report — when AI recommendations do not align with clinical observation.
Accountability: When an AI-assisted device makes a recommendation that leads to patient harm, who is responsible? Currently, legal and professional accountability frameworks have not fully resolved this question. Nurses must document their own clinical reasoning separately from AI outputs.
Transparency: Nurses should advocate for “explainable AI” — systems that communicate why they generate a specific alert or recommendation, not just what the recommendation is.
Practical Implementation Guide: Integrating Smart Devices Without Increasing Burnout
Step-by-Step Adoption Strategy
Step 1: Needs Assessment (Before Any Device Is Purchased) Survey nursing staff about current workflow pain points. Where is time lost? Where are errors occurring? Where is cognitive load highest? Technology should solve identified problems — not introduce solutions looking for problems.
Step 2: Staff Involvement in Device Selection Nurses must be represented in procurement committees. A device that looks efficient in a vendor demonstration may be impractical in actual ward conditions. Pilot testing with frontline nurses before full deployment is non-negotiable.
Step 3: Phased Implementation Roll out smart devices in phases — starting with one ward or unit. Evaluate the impact on workflow metrics (time-on-task, alert response rates, documentation burden) and burnout indicators (self-report scales, sick day frequency) before expanding.
Step 4: Training That Matches Clinical Reality Technology training for nurses must happen in clinical environments — not in conference rooms. Simulation-based training using actual device workflows produces better retention than slide-based instruction (McGaghie et al., 2011).
Step 5: Alarm Management Policy Before any monitoring device is activated, the hospital must have a written alarm management policy defining: default alarm thresholds, individualization parameters, escalation protocols, and audit review schedules.
Step 6: Ongoing Evaluation Smart device integration is not a one-time event. Establish quarterly reviews of device utilization data, nurse feedback, and clinical outcome metrics. Decommission devices that are not delivering intended benefits.
Budget Considerations for African Hospitals
Resource allocation in Ghanaian and broader Sub-Saharan African hospital settings requires creative approaches:
- Shared device models: High-cost monitors rotate across high-acuity patients rather than being assigned 1:1
- Donor and NGO partnerships: Organizations such as the World Health Organization, USAID, and GIZ have supported technology pilots in African hospitals
- Mobile-first approaches: Smartphone-based clinical apps require minimal hardware investment and can dramatically improve clinical decision support
- Government procurement frameworks: Ghana Health Service bulk procurement can reduce unit costs significantly
- Telemedicine grants: International and national grants targeting telehealth infrastructure can fund device acquisition indirectly
The Future of Nursing: Where Technology and Care Converge
Artificial Intelligence and Predictive Analytics
AI-driven predictive analytics represent the most transformative near-term opportunity for nursing workflow improvement. Platforms that analyze continuous vital signs, laboratory trends, and behavioral data to predict patient deterioration — such as sepsis, respiratory failure, or falls — before clinical signs appear give nurses actionable lead time.
The EarlySense system, for example, uses under-mattress sensors and AI to predict patient deterioration hours before traditional assessment would detect it. Studies show implementation reduced ICU transfers and pressure ulcer rates while decreasing nursing response burden (Zimlichman et al., 2012).
For Africa, where advanced diagnostic resources are frequently limited, AI that maximizes the clinical intelligence extractable from basic vital signs data is particularly valuable.
Smart Hospitals and the Internet of Medical Things (IoMT)
The Internet of Medical Things (IoMT) describes the ecosystem of connected medical devices — from wearables to infusion pumps to environmental sensors — that communicate via secure hospital networks. Smart hospitals built on IoMT infrastructure can automate medication dispensing, monitor environmental conditions (temperature, humidity in medication storage), track equipment location in real time, and generate population-level ward data for clinical governance.
African hospitals integrating IoMT infrastructure must prioritize network security architecture from the beginning — not as an afterthought. My background in network engineering makes me acutely aware of how many healthcare facilities deploy clinical devices on unsecured or poorly segmented networks, creating extraordinary vulnerability.
Robotics in Nursing
Nursing robotics remains largely nascent but is rapidly maturing. Current applications include:
- Medication dispensing robots (reducing pharmacist and nurse dispensing workload)
- Disinfection robots (UV-C automated room sterilization)
- Patient mobility assist robots (reducing musculoskeletal injury in nurses from patient lifting)
- Telepresence robots (enabling remote specialist consultation at the bedside)
For Sub-Saharan Africa, robotics adoption will initially be limited to major teaching hospitals and private sector facilities. However, the trajectory is clear — and nurses who understand these systems today will be positioned as leaders in their institutions tomorrow.
Telehealth and Remote Monitoring
COVID-19 accelerated global telehealth adoption by an estimated 38-fold in certain markets (McKinsey & Company, 2021). In Ghana, telemedicine has expanded through initiatives including the Ghana Telemedicine Program and various mobile health (mHealth) platforms targeting rural and peri-urban populations.
For nurses, telehealth integration means:
- Remote patient monitoring between clinic visits
- Virtual nursing assessments for stable patients
- Digital patient education platforms
- Cross-facility specialist consultation
African Healthcare Innovation: A Continent Rising
It would be a disservice to African healthcare to frame the continent purely as a recipient of technology from elsewhere. Ghana’s own healthcare innovation ecosystem is producing relevant solutions — from mobile diagnostic platforms to AI-assisted malaria diagnosis tools developed at Ghanaian institutions.
KNUST (Kwame Nkrumah University of Science and Technology) and the University of Ghana School of Medicine are producing health informatics researchers developing solutions designed for African clinical realities. Nurses across the continent are increasingly at the center of mHealth program design, recognizing that frontline nursing insight is irreplaceable in building technology that actually works in our environments.
FAQ: Smart Devices, Nursing Workflow, and Burnout
Q1: Is AI replacing nurses?
No. Artificial intelligence in healthcare is a tool — not a replacement for the clinical judgment, compassionate care, ethical reasoning, and physical presence that nursing requires. AI augments nursing by processing data at scale, identifying patterns, and reducing cognitive load for routine tasks. The irreplaceable human dimensions of nursing — assessment, advocacy, patient relationship, and adaptive decision-making — remain entirely within the nursing scope. Nurses who learn to work effectively alongside AI will be more effective clinicians, not less necessary ones.
Q2: Are wearable monitoring devices accurate enough for clinical use?
Consumer-grade wearables (e.g., basic fitness trackers) are generally not validated for clinical monitoring and should not be used for clinical decisions. Medical-grade wearables — those with FDA clearance or CE marking — have demonstrated clinical accuracy for SpO2, heart rate, and ECG in peer-reviewed validation studies. Always verify that any device used for clinical monitoring has appropriate regulatory clearance and published clinical validation data.
Q3: How can nurses protect patient data when using smart devices?
Follow the basic principles: use only hospital-approved, HIPAA/Act 843-compliant apps; never transmit patient information via unsecured personal messaging apps; lock device screens between use; attend cybersecurity training annually; report suspicious device behavior immediately; and always question vendors about their data security practices before adoption.
Q4: What apps are best for shift management?
NurseGrid and ShiftKey are widely used for shift scheduling and management in nurse-heavy environments. For Ghanaian nurses, Google Calendar with shift color-coding and Telegram-based unit communication (with awareness of its security limitations) are pragmatic low-cost alternatives. As institutional apps become more available, transitioning to hospital-managed platforms with proper data governance is recommended.
Q5: Are smart devices affordable in Ghana?
Affordability varies significantly by device category. Mobile clinical apps are the most accessible — many are free or low-cost and require only a smartphone. Clinical-grade wearables for nurses (smartwatches with clinical features) range from GHS 600–1200 for functional mid-range options. Patient monitoring smart devices and smart infusion pumps remain expensive and largely dependent on institutional procurement rather than individual nurse purchase.
Q6: How do smart devices specifically help with burnout reduction?
When implemented thoughtfully, smart devices reduce burnout by: decreasing repetitive physical tasks (e.g., continuous monitoring replaces hourly manual vitals); reducing cognitive load through clinical decision support; improving communication efficiency; and supporting nurse self-monitoring of physiological stress indicators. The critical condition is “thoughtful implementation” — poorly managed devices increase alert fatigue and worsen burnout.
Q7: What should a nurse do when a smart device malfunctions during patient care?
Revert immediately to manual clinical assessment — the gold standard. Never delay patient care while troubleshooting a device. Report the malfunction to biomedical engineering or IT immediately after the patient is stabilized. Document the malfunction and any impact on care in the patient record and in the hospital’s incident reporting system.
Q8: Can nurses advocate for better technology in their hospitals?
Absolutely — and they should. Nurses are the primary users of clinical technology, and their frontline insight is invaluable for procurement decisions. Formal channels include nursing unit management, hospital quality improvement committees, GRNMA advocacy platforms, and direct engagement with hospital administration. Evidence-based proposals — citing workflow impact data and clinical outcome improvements — are most effective.
Q9: Are smart devices safe in tropical and high-humidity environments like Ghana?
Not all smart devices are designed for tropical environments. When evaluating devices, check Ingress Protection (IP) ratings — IP54 or higher indicates resistance to dust and water splashing. Some monitoring devices have additional clinical-grade environmental specifications. Biomedical engineering staff should verify environmental suitability before deployment.
Q10: How does alert fatigue connect to patient safety?
Alert fatigue is directly linked to patient harm. When nurses become desensitized to device alarms due to overwhelming false-positive rates, true clinical emergencies risk being missed or delayed. A 2022 Joint Commission Sentinel Event Alert identified alarm fatigue as a top patient safety concern in hospitals globally. Effective alarm management — not alarm elimination — is the solution.
Q11: What is the nurse’s role in AI-assisted clinical decision support?
The nurse’s role is clinical judgment, oversight, and advocacy. AI-generated recommendations should be treated as clinical input — like a laboratory value or a consultant opinion — that informs but does not replace nursing assessment. Nurses must maintain the skill to independently assess patients and recognize when AI outputs are inconsistent with clinical observation. Documentation of independent clinical reasoning alongside AI recommendations protects both patient safety and nursing professional accountability.
Q12: How can nurses in rural Ghanaian postings benefit from smart devices?
Mobile-first solutions are most relevant for rural settings — clinical decision support apps, telemedicine consultation platforms, and mHealth tools for patient education and follow-up. Several Ghanaian and international organizations are piloting solar-powered tablet-based clinical decision support tools for rural health workers. The Ghana Health Service’s mHealth initiatives represent an ongoing pathway for rural nurses to access technology-enabled support.
Acknowledgements
To every nurse who has stood at a bedside at 3 AM, making decisions with limited resources and extraordinary skill — this article is for you.
My deepest appreciation goes to the Ghana Health Service for providing me with a clinical home and the opportunity to serve Ghanaian patients across emergency, intensive care, pediatric, and general ward settings for over a decade.
To my nursing mentors across the Emergency Department and ICU — your guidance shaped not only my clinical practice but my commitment to elevating the nursing profession through education and advocacy.
To the global nursing community — particularly frontline nurses in low- and middle-income countries navigating the double burden of resource limitation and rising patient complexity — your resilience is the foundation on which healthcare systems stand.
To the healthcare technology innovators who design with nurses in mind: keep listening to the frontline. The best technology in the world fails if it does not work at the bedside.
About the Author
Abdul-Muumin Wedraogo, RN, BSN
Abdul-Muumin Wedraogo is a Registered General Nurse with over 10 years of frontline clinical experience across Emergency, ICU, Pediatrics, and General Ward settings under the Ghana Health Service. He holds a Bachelor of Science in Nursing (BSN) alongside a Diploma in Network Engineering and an Advanced Professional certification in System Engineering.
He is a registered member of the Nurses and Midwifery Council (NMC) of Ghana and the Ghana Registered Nurses and Midwives Association (GRNMA).
His professional focus sits at the intersection of clinical nursing practice and healthcare technology — exploring how smart devices, mobile applications, AI, and cybersecurity frameworks can strengthen nursing care delivery, particularly in African healthcare contexts.
He writes at wadrago.com on topics including Nurse Lifestyle, Nurse Wellness, Nursing Technology, Cybersecurity for Nurses, and AI in Nursing.
References
Agyemang-Duah, W., Mensah, C. M., Peprah, P., & Arthur, F. (2021). Technological challenges facing healthcare workers in Ghana: A qualitative study. BMC Health Services Research, 21(1), 1–12. https://doi.org/10.1186/s12913-021-06500-6
Cornell, P., Riordan, M., Townsend-Gervis, M., & Mobley, R. (2011). Barriers to critical thinking: Workflow interruptions and task complexity in nursing practice. Journal of Nursing Administration, 41(10), 407–414. https://doi.org/10.1097/NNA.0b013e31822edd7e
Cvach, M. (2012). Monitor alarm fatigue: An integrative review. Biomedical Instrumentation & Technology, 46(4), 268–277. https://doi.org/10.2345/0899-8205-46.4.268
Downey, C. L., Randell, R., Brown, J., & Jayne, D. G. (2019). Continuous versus intermittent vital signs monitoring using a wearable, wireless patch in patients admitted to surgical wards: Pilot cluster randomized controlled trial. Journal of Medical Internet Research, 21(5), e13802. https://doi.org/10.2196/13802
Drew, B. J., Harris, P., Zègre-Hemsey, J. K., Mammone, T., Schindler, D., Salas-Boni, R., & Hu, X. (2014). Insights into the problem of alarm fatigue with physiologic monitor devices: A comprehensive observational study of consecutive intensive care unit patients. PLOS ONE, 9(10), e110274. https://doi.org/10.1371/journal.pone.0110274
Ghana Data Protection Commission. (2012). Data Protection Act, 2012 (Act 843). Government of Ghana. https://www.dataprotection.org.gh/
Grand View Research. (2023). Smart healthcare market size, share & trends analysis report. https://www.grandviewresearch.com/industry-analysis/smart-healthcare-market
Hicks, R. W., Becker, S. C., & Cousins, D. D. (2015). Nursing workload and medication errors. Nursing Management, 46(4), 24–30. https://doi.org/10.1097/01.NUMA.0000462384.78234.8e
IBM Security. (2023). Cost of a data breach report 2023. IBM Corporation. https://www.ibm.com/reports/data-breach
Institute for Safe Medication Practices. (2020). Smart infusion pumps: ISMP guidelines for optimizing safe implementation and use in hospitals. ISMP. https://www.ismp.org/
Joint Commission. (2022). Sentinel event alert: Medical device alarm safety in hospitals. The Joint Commission. https://www.jointcommission.org/
Keller, S., Tschan, F., Semmer, N. K., Timm-Holzer, E., Zimmermann, J., Candinas, D., & Beldi, G. (2020). “Disruptive” interruptions of nurses’ work: An observational study in hospitals. Journal of Nursing Management, 28(3), 584–591. https://doi.org/10.1111/jonm.12951
Labrague, L. J., de los Santos, J. A. A., & Fronda, D. C. (2022). Factors associated with missed nursing care and nurse‐assessed quality of care during the COVID‐19 pandemic. Journal of Nursing Management, 30(1), 62–70. https://doi.org/10.1111/jonm.13483
McGaghie, W. C., Issenberg, S. B., Cohen, E. R., Barsuk, J. H., & Wayne, D. B. (2011). Does simulation-based medical education with deliberate practice yield better results than traditional clinical education? A meta-analytic comparative review of the evidence. Academic Medicine, 86(6), 706–711. https://doi.org/10.1097/ACM.0b013e318217e119
McKinsey & Company. (2021). Telehealth: A quarter-trillion-dollar post-COVID-19 reality? https://www.mckinsey.com/industries/healthcare/our-insights/telehealth-a-quarter-trillion-dollar-post-covid-19-reality
Nuckols, T. K., Bower, A. G., Paddock, S. M., Hilborne, L. H., Wallace, P., Rothschild, J. M., & Asch, S. M. (2016). Programmable infusion pumps in ICUs: An analysis of corresponding adverse drug events. Journal of General Internal Medicine, 21(S3), S35–S39. https://doi.org/10.1111/j.1525-1497.2006.00614.x
Poissant, L., Pereira, J., Tamblyn, R., & Kawasumi, Y. (2005). The impact of electronic health records on time efficiency of physicians and nurses: A systematic review. Journal of the American Medical Informatics Association, 12(5), 505–516. https://doi.org/10.1197/jamia.M1700
Sweller, J. (1988). Cognitive load during problem solving: Effects on learning. Cognitive Science, 12(2), 257–285. https://doi.org/10.1207/s15516709cog1202_4
World Health Organization. (2023). Global strategic directions for nursing and midwifery 2021–2025. WHO Press. https://www.who.int/publications/i/item/9789240033863
Zimlichman, E., Henderson, D., Tamir, O., Franz, C., Song, P., Yamin, C. K., & Bates, D. W. (2012). Health care-associated infections: A meta-analysis of costs and financial impact on the US health care system. JAMA Internal Medicine, 173(22), 2039–2046. https://doi.org/10.1001/jamainternmed.2013.9763
© Abdul-Muumin Wedraogo, RN, BSN | wadrago.com | All rights reserved
For permissions, collaboration, or citation inquiries: contact via wadrago.com