A registered nurse with 10+ years of ICU/ER experience breaks down 12-lead ECG interpretation for nurses — from rhythm basics to life-threatening arrhythmias, with clinical pearls.
| ABOUT THE AUTHOR By Abdul-Muumin Wedraogo, BSN, RN, Registered General Nurse | Ghana Health Service | 10+ Years Clinical Experience (ER, ICU, Pediatrics, General Ward) Abdul-Muumin Wedraogo is a Registered General Nurse with over 10 years of hands-on clinical experience across emergency, intensive care, pediatric, and general ward settings in Ghana. He holds a Bachelor of Science in Nursing from Valley View University and a Nursing Diploma from Premier Nurses’ Training College. He is a member of both the Nurses and Midwifery Council (NMC) Ghana and the Ghana Registered Nurses and Midwives Association (GRNMA).In his daily clinical work, Abdul-Muumin frequently interprets 12-lead ECGs as a frontline tool in patient assessment. He writes about cardiac monitoring because he has seen, first-hand, how fast and accurate ECG interpretation saves lives in under-resourced settings. His combined background in nursing and systems engineering gives him a uniquely practical approach to clinical technology. Last Reviewed: May 2026 | Estimated Reading Time: 20–25 minutes |
⚠️ Medical Disclaimer: This content is for informational and educational purposes only and does not replace professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare provider for clinical decisions.
Table of Contents
1. Introduction: A Monitor That Changed Everything
It was a Tuesday afternoon in our general ward when a 58-year-old man — I’ll call him Mr. Kofi — was brought in complaining of mild dizziness and “a fluttering in the chest.” His blood pressure was acceptable, oxygen saturation was 97%, and to a less experienced eye, he looked fairly stable. But the moment I ran the 12-lead ECG, everything changed. The strip showed a classic irregular rhythm with absent P waves and an uncontrolled ventricular rate pushing 140 beats per minute. It was atrial fibrillation with rapid ventricular response, and Mr. Kofi was at imminent risk of hemodynamic compromise.
That strip — those 10 seconds of electrical recording — redirected his entire clinical course. Rate control was initiated, anticoagulation was considered, and a cardiologist was involved within the hour. Mr. Kofi was eventually discharged four days later, stable and informed. That is the power of 12-lead ECG interpretation, and it is why I believe every nurse working in a clinical setting needs to be fluent in reading it.
12-lead ECG interpretation is not a skill reserved for cardiologists. In hospitals across Ghana and around the world, nurses are often the first to place the electrodes, the first to see the tracing, and frequently the first to recognize that something is wrong. The ability to identify a dangerous arrhythmia, differentiate a benign rhythm variant from a life-threatening one, and communicate findings accurately to a physician is a core competency that saves lives.
In this guide, I will walk you through the foundations of 12-lead ECG interpretation, cover the most common arrhythmias you will encounter in clinical practice, provide a systematic approach you can use at the bedside, and share clinical pearls I have gathered across 10 years in emergency, ICU, pediatric, and general ward settings. Whether you are a nursing student, a new graduate, or an experienced clinician looking to sharpen your skills, this article is written with you in mind.
By the end of this post, you will be able to interpret a 12-lead ECG systematically, recognize the most clinically significant arrhythmias, understand when to escalate care immediately, and communicate your findings with confidence.
2. What You Need to Know About 12-Lead ECG Interpretation: A Clinical Perspective
The electrocardiogram has been a cornerstone of cardiac assessment since its clinical introduction in the early 20th century. Today, the 12-lead ECG remains the single most commonly performed cardiac diagnostic test worldwide, and for good reason: it is fast, non-invasive, inexpensive, and extraordinarily informative when interpreted correctly (American Heart Association, 2023).
Cardiovascular disease is the leading cause of death globally. According to the World Health Organization (2024), an estimated 17.9 million people die from cardiovascular diseases each year, accounting for 32% of all global deaths. In Ghana specifically, cardiovascular conditions are among the top causes of hospital admission and mortality, particularly in adult and elderly populations (Ghana Health Service, 2023). Arrhythmias, whether detected in isolation or in the context of acute coronary syndromes or cardiomyopathies, represent a significant proportion of those cases.
Despite its importance, 12-lead ECG interpretation is a skill that many nurses feel underprepared to use. A survey published in the Journal of Clinical Nursing found that fewer than 30% of registered nurses felt confident interpreting complex arrhythmias without physician support ([Riesenberg et al., 2023]. This gap in confidence is not a reflection of nursing intelligence — it reflects inadequate training, limited supervised practice, and the intimidating jargon that surrounds cardiac electrophysiology.
The standard 12-lead ECG records electrical activity from 12 different anatomical perspectives simultaneously: six limb leads (I, II, III, aVR, aVL, aVF) and six precordial or chest leads (V1 through V6). Each lead captures the heart’s electrical events from a unique angle, giving a three-dimensional picture of cardiac conduction. This spatial richness allows clinicians to localize ischemia, identify conduction abnormalities, and characterize rhythm disturbances far more precisely than a single-lead rhythm strip.
Clinical guidelines from the American Heart Association and the European Society of Cardiology recommend that all clinical nurses working in emergency, intensive care, and acute care settings receive formal ECG interpretation training as part of their core competencies ([AHA, 2023]; [ESC, 2023]). In many high-income countries, Advanced Cardiac Life Support (ACLS) certification, which includes rhythm recognition, is mandatory for ICU and ER nurses. In lower-resource settings like many parts of sub-Saharan Africa, nurses carry an even greater responsibility because cardiologists may not always be immediately available.
The evolution of ECG technology has also been remarkable. From paper-based recordings requiring manual measurement to digital systems with built-in interpretation algorithms, modern ECG machines do a great deal of the computational work. But algorithms are not infallible — studies have shown that automated ECG interpretations carry a significant error rate, particularly for complex arrhythmias and ST changes [Schlapfer & Wellens, 2017, JACC]. A skilled human eye, trained to recognize patterns and integrate clinical context, remains irreplaceable.
3. ECG Basics Every Nurse Must Know
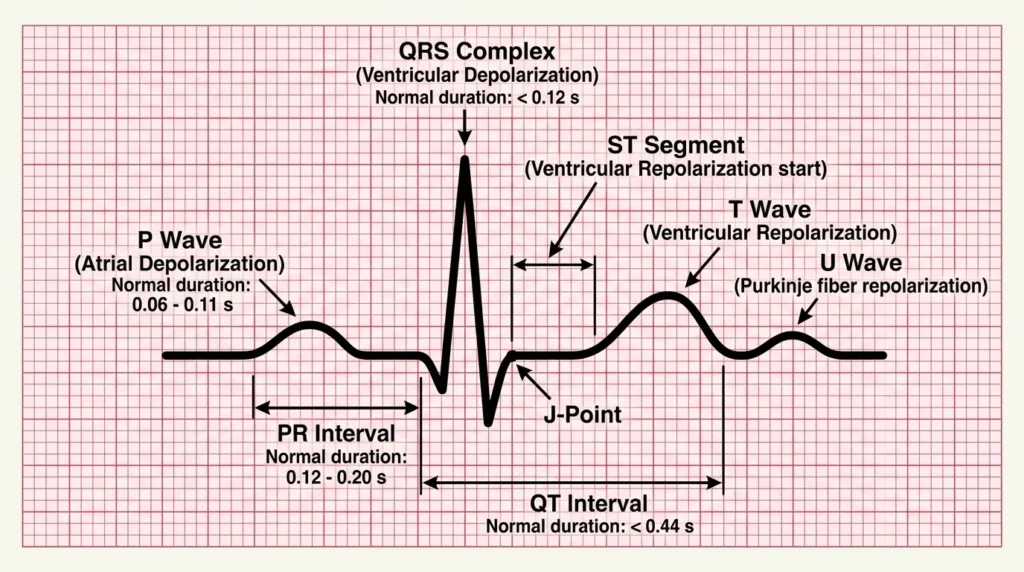
Before diving into specific arrhythmias, it is essential to have a firm grasp of the ECG waveform components. Think of the ECG as a musical score: each wave, interval, and segment represents a specific electrical event in the cardiac cycle. Missing or misreading one note changes the entire meaning of the piece.
The Cardiac Conduction System
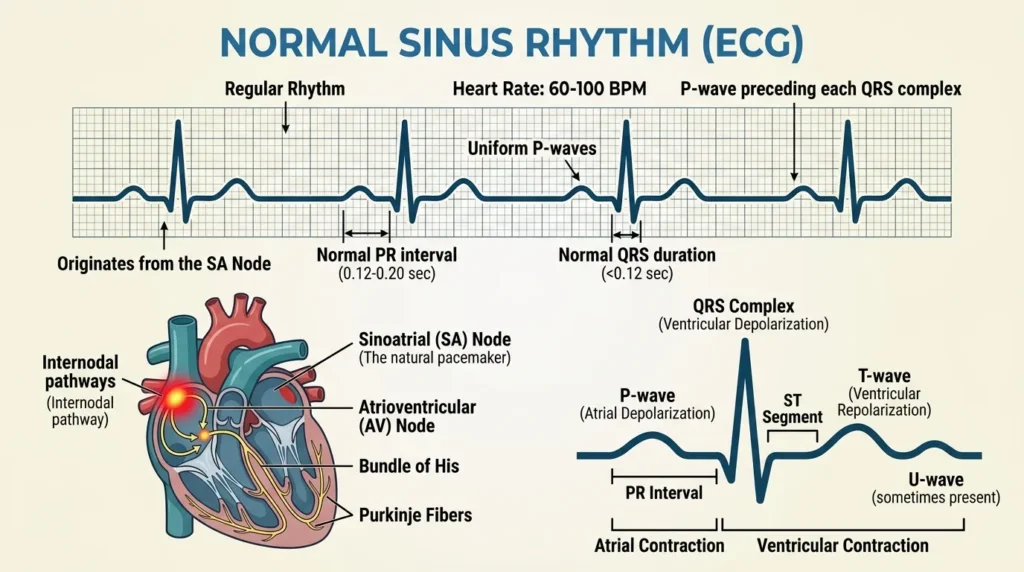
The heart’s electrical impulse originates in the sinoatrial (SA) node in the right atrium, travels through the atria (producing the P wave), reaches the atrioventricular (AV) node where it pauses briefly to allow ventricular filling, then descends rapidly through the Bundle of His, the left and right bundle branches, and finally the Purkinje fibers to activate the ventricles (producing the QRS complex). Ventricular repolarization follows, producing the T wave. Any disruption anywhere along this highway produces a recognizable change on the ECG tracing.
Key ECG Waveform Components
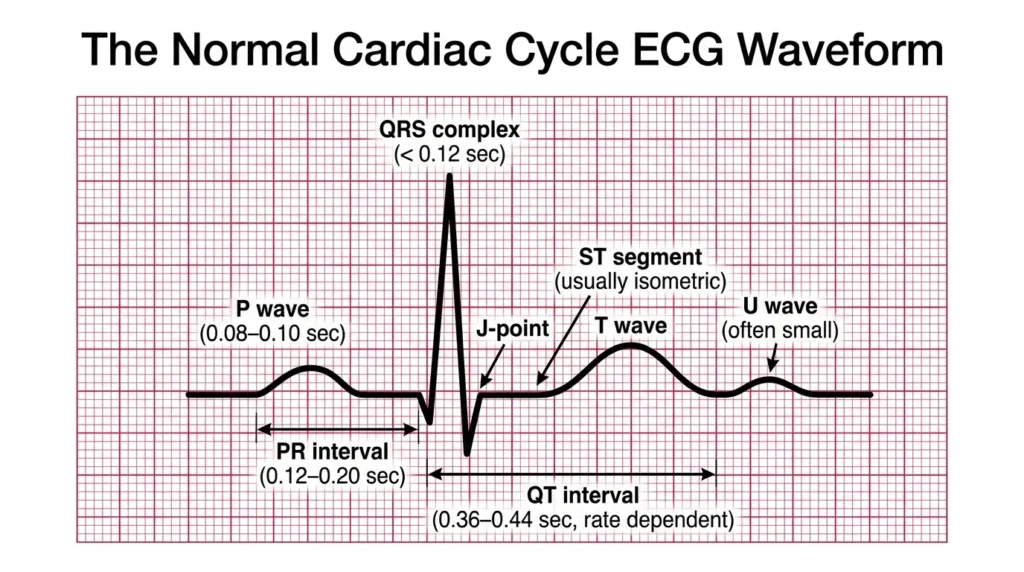
- P Wave: Represents atrial depolarization. Normally upright in leads I, II, and aVF, less than 2.5 mm tall, and less than 120 ms (3 small squares) in duration. Absent P waves suggest atrial fibrillation or junctional rhythms. Inverted P waves may indicate an ectopic atrial focus or retrograde conduction.
- PR Interval: Measured from the start of the P wave to the start of the QRS complex. Normal range is 120–200 ms (3–5 small squares). A PR interval greater than 200 ms indicates AV block. A short PR with a delta wave suggests an accessory pathway (Wolff-Parkinson-White syndrome).
- QRS Complex: Represents ventricular depolarization. Normal duration is less than 120 ms (3 small squares). A wide QRS (>120 ms) suggests a bundle branch block, ventricular origin of the rhythm, or aberrant conduction. The QRS morphology helps identify ischemia, hypertrophy, and conduction abnormalities.
- ST Segment: The flat segment between the end of the QRS (J-point) and the start of the T wave. Should sit at the isoelectric baseline. ST elevation greater than 1 mm in two contiguous limb leads or greater than 2 mm in precordial leads is pathological and raises concern for acute myocardial infarction or pericarditis. ST depression suggests ischemia or posterior MI.
- T Wave: Represents ventricular repolarization. Should be upright in most leads except aVR and V1. T-wave inversions may indicate ischemia, right ventricular strain, or digitalis effect. Tall, peaked T waves can indicate hyperkalemia.
- QT/QTc Interval: Measured from the start of the QRS to the end of the T wave. The corrected QT interval (QTc) accounts for heart rate and should be less than 440 ms in men and less than 460 ms in women. A prolonged QTc predisposes to Torsades de Pointes, a dangerous ventricular arrhythmia.
Paper Speed and Grid Understanding
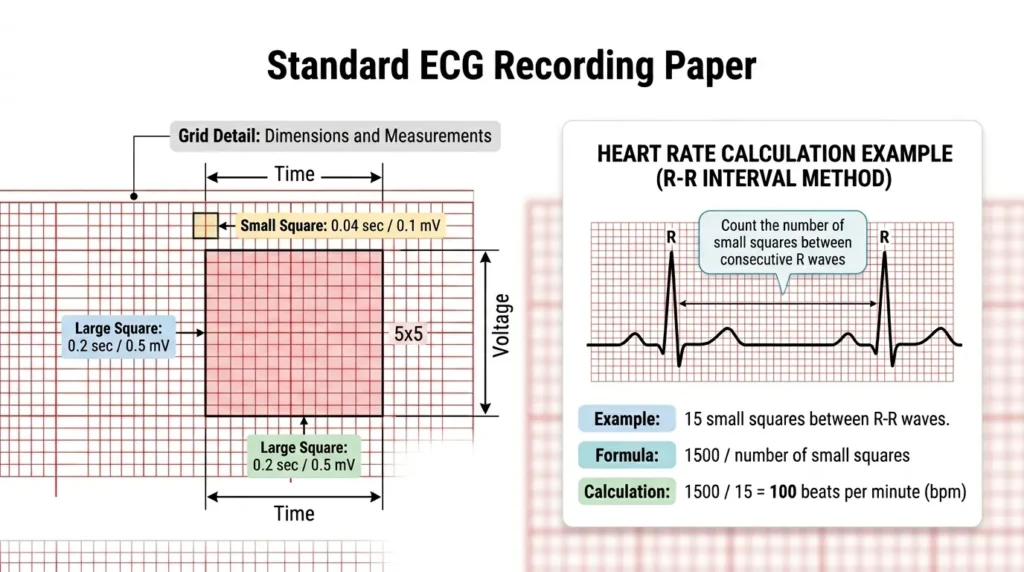
Standard ECG paper runs at 25 mm per second. Each small square on the ECG grid represents 0.04 seconds (40 ms) horizontally and 0.1 mV vertically. Five small squares make one large square, representing 0.2 seconds. Twenty-five large squares represent one second. Knowing this allows you to calculate heart rate, measure intervals, and assess amplitude accurately without specialized equipment.
Quick Heart Rate Calculation: Count the number of large squares between two consecutive R waves. Divide 300 by that number to get the approximate heart rate. For example, if there are 4 large squares between R waves, the heart rate is approximately 300 ÷ 4 = 75 bpm. For irregular rhythms, count the number of QRS complexes in a 6-second rhythm strip and multiply by 10.
4. Systematic 12-Lead ECG Interpretation: A Step-by-Step Framework
One of the most valuable things I learned during my ICU rotations was to approach every single ECG the same way, regardless of the clinical urgency. A systematic method prevents tunnel vision, where you fixate on one abnormality and miss another. Here is the structured approach I use and teach to junior nurses.
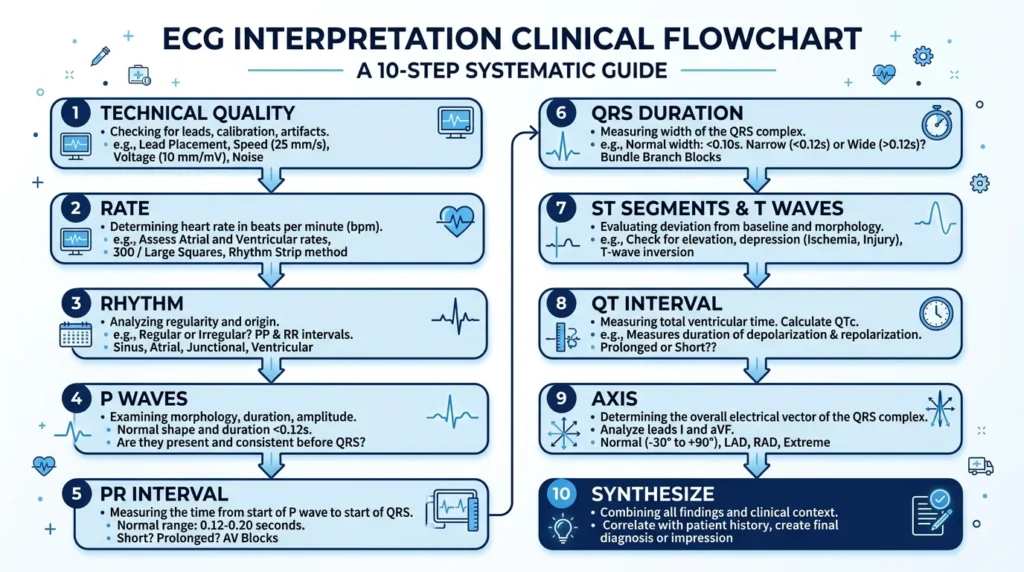
Step 1: Confirm Technical Quality
Before interpreting anything, verify that the ECG is technically adequate. Check for lead placement errors (reversed limb leads produce characteristic patterns), baseline artifact (motion or muscle tremor), and adequate electrode contact. A poor-quality tracing can mimic or mask arrhythmias. I have seen junior nurses call arrhythmias on leads that were simply poorly attached.
Step 2: Determine the Rate
Calculate the ventricular rate as described above. Is it normal (60–100 bpm), bradycardic (<60 bpm), or tachycardic (>100 bpm)? The rate provides your first major clinical category.
Step 3: Assess the Rhythm
Is the rhythm regular or irregular? Use calipers or the paper-and-pencil method to compare R-R intervals across the strip. Irregular rhythms can be regularly irregular (a predictable pattern, as in second-degree AV block) or irregularly irregular (no pattern, as in atrial fibrillation). This distinction is critical.
Step 4: Examine the P Waves
Are P waves present? If yes, are they upright in leads I and II? Is there one P wave before every QRS? Do all P waves look the same? Multiple P wave morphologies suggest multifocal atrial tachycardia. Absent P waves with a fine irregular baseline suggest atrial fibrillation. Sawtooth P waves at approximately 300 bpm are pathognomonic of atrial flutter.
Step 5: Measure the PR Interval
Is the PR interval within normal limits (120–200 ms)? Does it remain constant or does it vary? A progressively lengthening PR that culminates in a dropped QRS is Mobitz Type I (Wenckebach) second-degree AV block. A constant PR with suddenly dropped QRS beats is Mobitz Type II, a more dangerous entity.
Step 6: Measure the QRS Duration and Morphology
Is the QRS narrow (<120 ms) or wide (>120 ms)? A wide QRS indicates either ventricular origin, bundle branch block, or aberrant conduction. Right bundle branch block (RBBB) produces an RSR’ (“rabbit ears”) pattern in V1 and a wide, slurred S wave in lateral leads. Left bundle branch block (LBBB) produces a broad, notched R in lateral leads and a deep S in V1. Distinguishing LBBB from RBBB has major clinical implications.
Step 7: Assess the ST Segments and T Waves
Scan all 12 leads methodically for ST elevation, ST depression, and T-wave inversions. Document which leads are affected and whether they follow a coronary artery distribution. Remember: ST changes must be interpreted in the clinical context. Benign early repolarization can mimic STEMI in young patients, and digitalis effect produces a distinctive scooping of the ST segment.
Step 8: Measure the QT Interval
Calculate the QTc, particularly in patients receiving antiarrhythmics, antibiotics (fluoroquinolones, azithromycin), antipsychotics, or those with electrolyte abnormalities. A QTc above 500 ms warrants urgent physician notification and medication review.
Step 9: Identify the Axis
Although axis calculation can feel complex, a quick assessment is possible. A normal axis falls between -30 and +90 degrees. If leads I and aVF are both upright, the axis is normal. Left axis deviation (negative aVF, positive I) may indicate left anterior fascicular block. Right axis deviation (positive aVF, negative I) may suggest right ventricular hypertrophy, pulmonary hypertension, or lateral MI.
Step 10: Synthesize and Contextualize
Finally, integrate all your findings with the patient’s clinical presentation, vital signs, symptoms, and history. An ECG never exists in isolation. A rhythm that looks like VT in an asymptomatic patient receiving beta-blockers requires a very different response than the same rhythm in a haemodynamically unstable patient clutching their chest. Always communicate your findings clearly to the responsible physician.
5. Common Arrhythmias in Clinical Practice
Here, I will walk through the most common arrhythmias you will encounter as a nurse, with ECG characteristics, clinical significance, and practical nursing considerations for each.
5.1 Sinus Bradycardia and Sinus Tachycardia
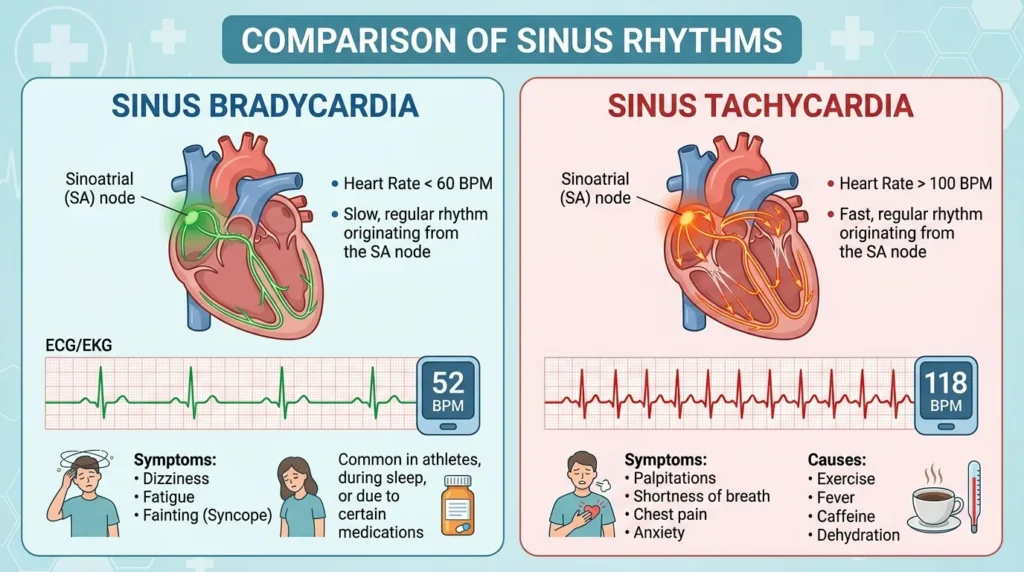
Sinus Bradycardia
Sinus bradycardia is defined as a sinus rhythm with a rate below 60 beats per minute. The ECG shows normal P waves, a normal PR interval, a normal QRS complex, and a regular rhythm — just slower than usual. In athletes and well-conditioned individuals, sinus bradycardia is a normal variant and carries no clinical concern. In hospitalized patients, however, it can signal hypothyroidism, increased intracranial pressure, inferior myocardial infarction (through vagal stimulation), medication effects (beta-blockers, calcium channel blockers, digoxin), or sick sinus syndrome.
From a nursing standpoint, the critical question is always: Is the patient symptomatic? A heart rate of 48 bpm in a sleeping patient who is hemodynamically stable requires monitoring. That same rate in a patient who is dizzy, diaphoretic, and hypotensive requires immediate intervention. The ACLS algorithm for symptomatic bradycardia includes atropine 0.5 mg IV (up to 3 mg), transcutaneous pacing, and dopamine or epinephrine infusion if atropine is ineffective [AHA, 2020 ACLS Guidelines].
In my ER experience, I have cared for several patients where beta-blocker toxicity caused profound bradycardia, as low as 28 bpm in one case. The ECG was unmistakable: slow rate, otherwise normal morphology. The treatment in that case escalated to glucagon, high-dose insulin therapy, and ultimately lipid emulsion therapy. Recognizing the rhythm early allowed for faster escalation.
- Clinical Pearl: Always check the medication list when you encounter bradycardia. Beta-blockers, calcium channel blockers, digoxin, and amiodarone are the most common pharmacological culprits.
Sinus Tachycardia
Sinus tachycardia is a sinus rhythm with a rate above 100 bpm, characterized by normal P waves, normal PR interval, normal QRS morphology, and a regular rhythm. Unlike most other tachyarrhythmias, sinus tachycardia is almost always a secondary phenomenon — a physiological response to an underlying cause rather than a primary arrhythmia.
Common causes include fever, pain, anxiety, hypovolemia, anemia, hyperthyroidism, pulmonary embolism, and heart failure. In pediatric patients, it is important to know normal age-specific heart rates, as what constitutes tachycardia in an adult may be entirely normal in a child. In my pediatric ward rotations, I learned to approach tachycardia in children with a broad differential, particularly including dehydration and sepsis.
Treatment of sinus tachycardia is directed at the underlying cause, not the rate itself. Giving rate-controlling medications for sinus tachycardia due to hypovolemia, for example, can be catastrophically dangerous by removing the compensatory mechanism the body is relying upon.
- Clinical Pearl: The presence of sinus tachycardia in a postoperative patient should always prompt assessment for bleeding, pain, hypovolemia, and pulmonary embolism before any other intervention.
5.2 Atrial Fibrillation: The Most Common Sustained Arrhythmia
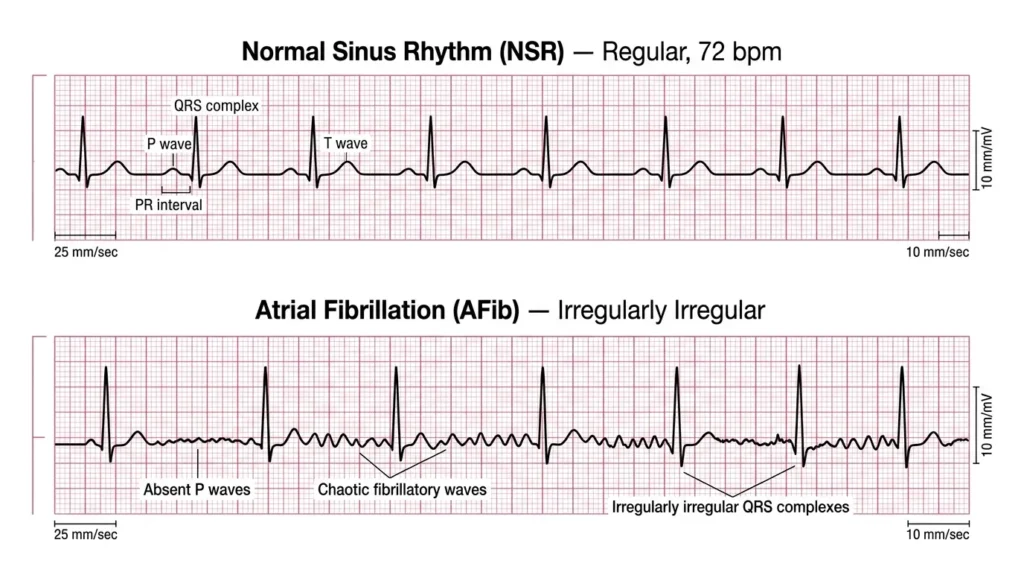
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia worldwide, affecting an estimated 37.5 million people globally ([Hindricks et al., ESC Guidelines, 2021]. The prevalence increases sharply with age, from less than 1% in individuals under 60 to over 10% in those over 80. In my clinical experience, AF is arguably the arrhythmia nurses will encounter most frequently in general wards and emergency settings.
The ECG hallmarks of atrial fibrillation are the absence of distinct P waves (replaced by a chaotic, irregular fibrillatory baseline) and an irregularly irregular ventricular response. The QRS complex is typically narrow unless aberrant conduction or a bundle branch block is present. Heart rate can vary widely — the ventricular response may be controlled (<100 bpm), uncontrolled (>100 bpm), or even slow if there is concomitant AV nodal disease or nodal-blocking medications.
The clinical consequences of AF are twofold. First, the loss of coordinated atrial contraction reduces cardiac output by approximately 15–20%, which can precipitate hemodynamic deterioration, particularly in patients with diastolic dysfunction. Second, stasis of blood in the left atrial appendage creates thrombi that can embolize to the cerebral circulation, causing ischemic stroke. AF accounts for approximately one in five strokes [Stroke Association, 2023].
Nursing management of AF involves monitoring hemodynamic stability, administering rate-controlling agents (beta-blockers, diltiazem, digoxin) or rhythm-controlling agents as prescribed, ensuring anticoagulation is in place per stroke risk stratification (CHA₂DS₂-VASc score), and monitoring for signs of decompensation. In hemodynamically unstable AF, synchronized cardioversion is indicated.
- Clinical Pearl: An irregularly irregular rhythm is almost always AF until proven otherwise. Do not accept a “normal ECG” read-out from the machine without verifying the rhythm yourself — automated algorithms frequently miss or misclassify AF.
5.3 Atrial Flutter
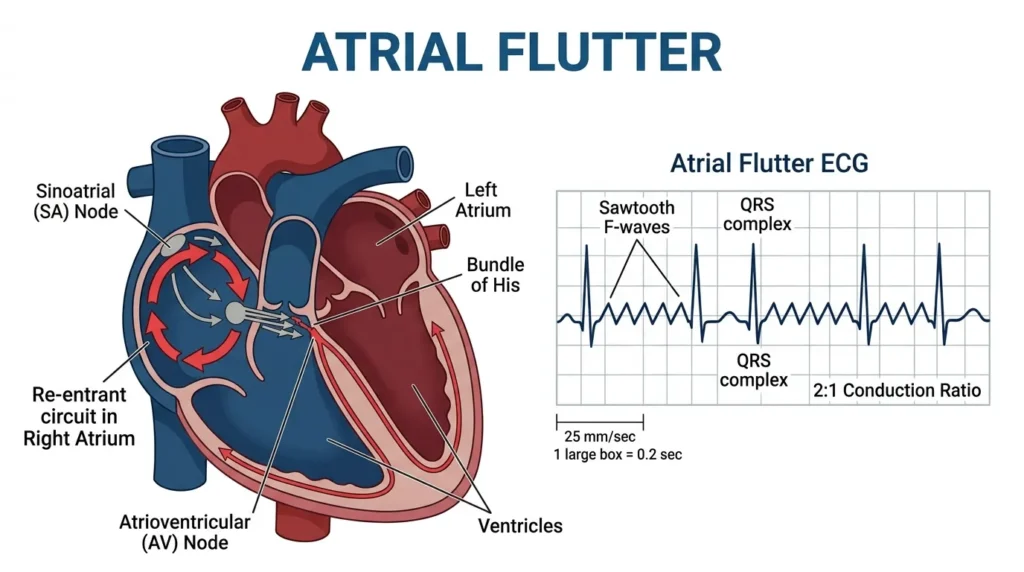
Atrial flutter is a macro-reentrant atrial arrhythmia in which the atria fire at approximately 300 beats per minute in a characteristic sawtooth pattern, most visible in the inferior leads (II, III, aVF) and in V1. The AV node cannot conduct all 300 impulses, so it typically conducts every second impulse (2:1 block), resulting in a ventricular rate of approximately 150 bpm, or every third (3:1) or fourth (4:1) impulse, resulting in slower ventricular rates.
The classic ECG appearance is a regular rhythm at approximately 150 bpm with no visible P waves but a sawtooth flutter wave baseline. If you ever see a regular tachycardia at exactly 150 bpm, atrial flutter with 2:1 block should be your first thought. I have seen this mistaken for sinus tachycardia more than once, with potentially dangerous consequences for management.
Atrial flutter carries the same stroke risk as AF and is managed similarly with rate control, rhythm control, and anticoagulation. Radiofrequency catheter ablation of the cavotricuspid isthmus is highly effective and curative for typical atrial flutter [Page et al., AHA/ACC Guidelines, 2019].
- Clinical Pearl: If you see a regular tachycardia at 150 bpm, apply gentle vagal maneuvers or adenosine under physician direction. Slowing the ventricular rate will unmask the sawtooth flutter waves and confirm the diagnosis.
5.4 Supraventricular Tachycardia (SVT)
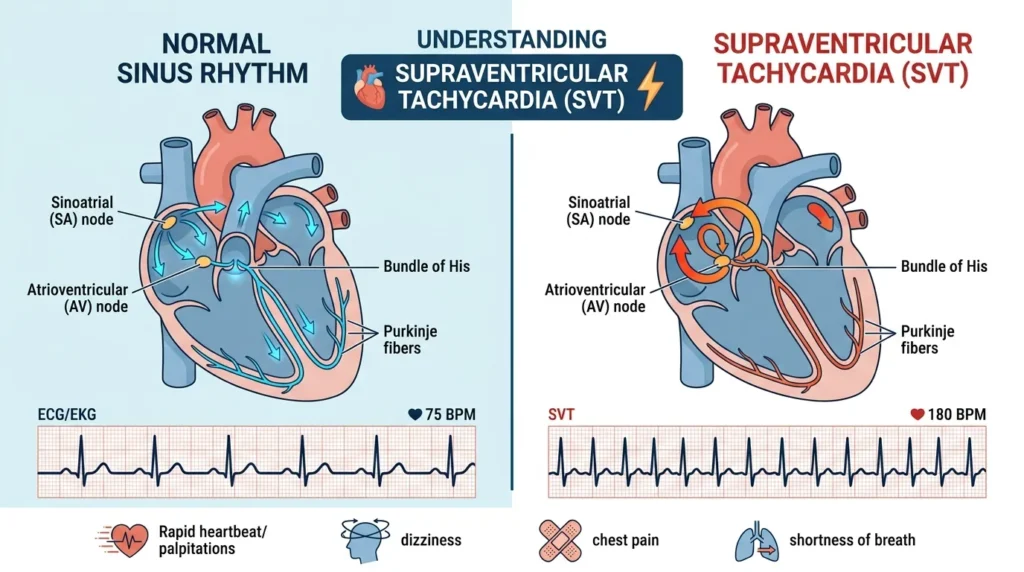
The term “supraventricular tachycardia” encompasses a group of tachyarrhythmias originating above the bundle of His. In clinical parlance, when nurses say SVT, they most often refer to AV nodal reentrant tachycardia (AVNRT), the most common form, which produces a regular, narrow-complex tachycardia at 150–250 bpm with absent or retrograde P waves that may appear just after the QRS complex or be buried within it.
SVT typically presents as sudden-onset palpitations, lightheadedness, and sometimes chest tightness or dyspnea. It can occur in patients of any age, including young adults with no structural heart disease. In my experience, SVT is one of the more anxiety-provoking rhythms for both the patient and the nursing staff because of its rapid onset and dramatic symptom presentation.
First-line management includes vagal maneuvers (Valsalva, modified Valsalva, carotid sinus massage in appropriate candidates) and, if unsuccessful, intravenous adenosine 6 mg rapid push, followed by 12 mg if needed [Page et al., AHA/ACC, 2019]. Adenosine transiently blocks the AV node and terminates reentrant circuits that depend on it. Nurses must warn patients that adenosine causes a brief, intensely uncomfortable sensation of chest heaviness and flushing. Reassurance matters enormously here.
- Clinical Pearl: Adenosine has an extremely short half-life of approximately 10 seconds. It must be given as a rapid IV push followed immediately by a 20 mL normal saline flush, ideally through an antecubital or larger vein. A slow push will be ineffective.
5.5 AV Heart Blocks: First, Second, and Third Degree
AV blocks represent impaired conduction through the atrioventricular node or His-Purkinje system. They range from the benign and clinically insignificant to the immediately life-threatening.
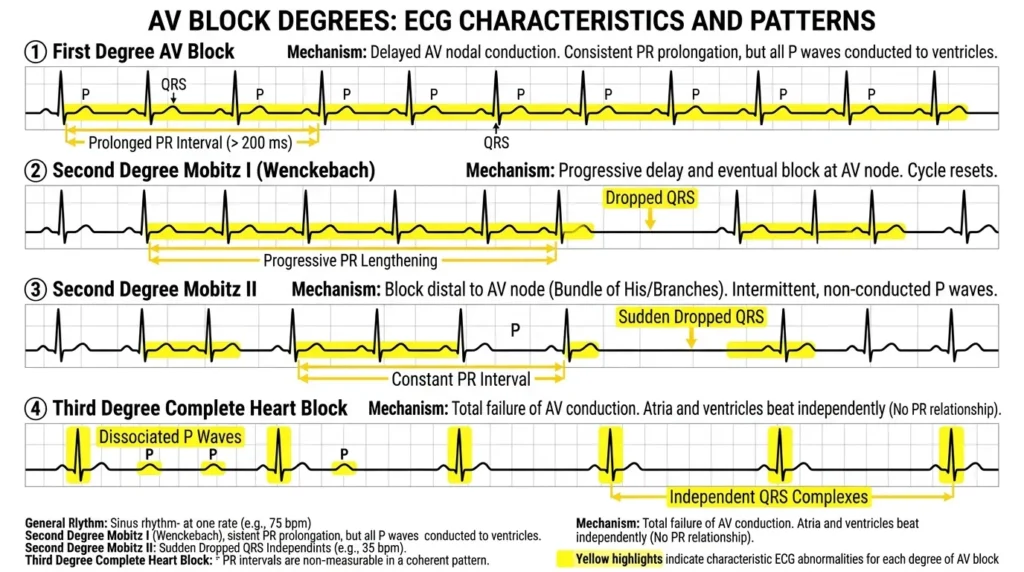
First Degree AV Block
First-degree AV block is defined as a PR interval greater than 200 ms (5 small squares) with every P wave still conducting to a QRS complex. The rhythm is regular, and P waves are present before every QRS. This is not truly a “block” in the sense of dropped beats — it reflects slowed conduction through the AV node.
First-degree AV block is commonly seen in athletes, elderly patients, and those on nodal-blocking medications. It rarely requires specific treatment unless it is new and associated with symptoms or progresses to a higher degree of blockage. However, in the context of inferior MI, new first-degree AV block may herald progression to complete heart block and warrants close monitoring.
Second Degree AV Block — Mobitz Type I (Wenckebach)
In Mobitz Type I block, the PR interval progressively lengthens with each beat until a P wave fails to conduct and the QRS is dropped. After the pause, the cycle restarts. This pattern is called Wenckebach periodicity. The ventricular rhythm is irregularly irregular. The block is typically within the AV node itself and is often benign, particularly in the context of inferior MI or increased vagal tone.
Management is generally conservative — monitoring, correction of reversible causes, and atropine for symptomatic patients. It rarely progresses to complete heart block, though careful observation is warranted in the acute MI setting.
Second Degree AV Block — Mobitz Type II
Mobitz Type II is significantly more dangerous. Here, the PR interval remains constant, but P waves suddenly fail to conduct without warning, producing dropped QRS beats. The block is typically at or below the Bundle of His, making progression to complete heart block both possible and unpredictable.
The QRS complex in Mobitz II is frequently wide due to bundle branch disease in the same region. Any patient with Mobitz II should be assumed to be at high risk of deteriorating to complete heart block and should be managed in a monitored setting with transcutaneous pacing readily available. Permanent pacemaker implantation is frequently indicated [Kusumoto et al., ACC/AHA Pacemaker Guidelines, 2018].
Third Degree (Complete) AV Block
In complete heart block, there is total dissociation between atrial and ventricular activity. The SA node fires at its intrinsic rate, P waves march across the strip at one rate, and a ventricular escape rhythm fires independently at 20–45 bpm (junctional escape) or even slower (ventricular escape). There is no relationship between P waves and QRS complexes.
The ECG shows P waves and QRS complexes that appear to “walk through” each other without consistent timing. The QRS morphology depends on the escape focus: junctional escapes are narrow, ventricular escapes are wide and bizarre.
Complete heart block is a cardiovascular emergency. Patients present with syncope, hemodynamic instability, altered consciousness, or cardiac arrest. Immediate management includes transcutaneous pacing while preparing for transvenous pacing, atropine (which may have a limited effect with infranodal blocks), and expert consultation. Permanent pacing is definitive therapy in most cases.
- Clinical Pearl: In complete heart block, the ventricular rate may appear “regular” at a slow rate. Do not be falsely reassured by the regular rhythm — the rate, the dissociation from P waves, and the wide QRS morphology are the red flags that demand immediate action.
5.6 Ventricular Tachycardia: Recognizing a Killer
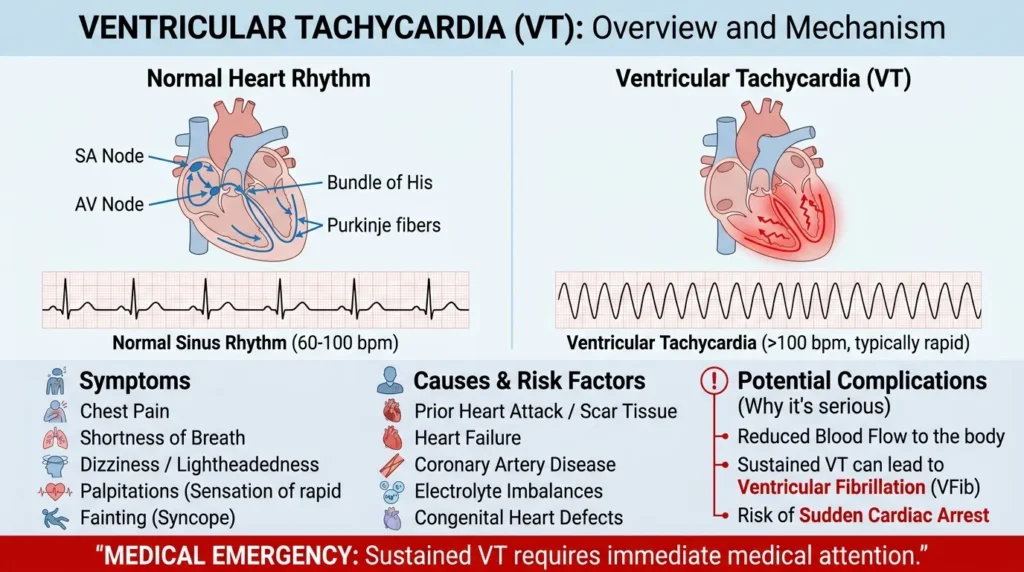
Ventricular tachycardia (VT) is a wide-complex tachycardia originating from the ventricles, with a rate typically between 100 and 250 bpm. It is one of the most life-threatening arrhythmias nurses will encounter, and the ability to rapidly recognize it can directly determine whether a patient lives or dies.
The ECG in VT shows a wide QRS (>120 ms) tachycardia, typically regular, with dissociated P waves that may be visible marching independently through the QRS complexes — a phenomenon called AV dissociation. Fusion beats (a hybrid between a sinus and a ventricular beat) and capture beats (a normally narrow QRS amidst the wide-complex tachycardia) are virtually diagnostic of VT when present.
A critical concept: any wide-complex tachycardia should be treated as VT until proven otherwise. The consequences of treating VT with AV nodal blockers (like verapamil or diltiazem) — appropriate for SVT with aberrancy — can be catastrophic in true VT, potentially precipitating VF and cardiac arrest. When in doubt, assume VT.
Management depends on hemodynamic stability. Stable VT may be treated with amiodarone 150 mg IV over 10 minutes or procainamide. Unstable VT with a pulse requires synchronized cardioversion. Pulseless VT is treated identically to ventricular fibrillation — immediate CPR and defibrillation per ACLS protocols [AHA ACLS, 2020].
- Clinical Pearl: The Brugada criteria and Vereckei algorithm are validated tools for differentiating VT from SVT with aberrancy. Familiarize yourself with them. But in urgent clinical scenarios, wide + fast + hemodynamic instability = treat as VT and call for help immediately.
5.7 Ventricular Fibrillation: Respond, Don’t Analyze
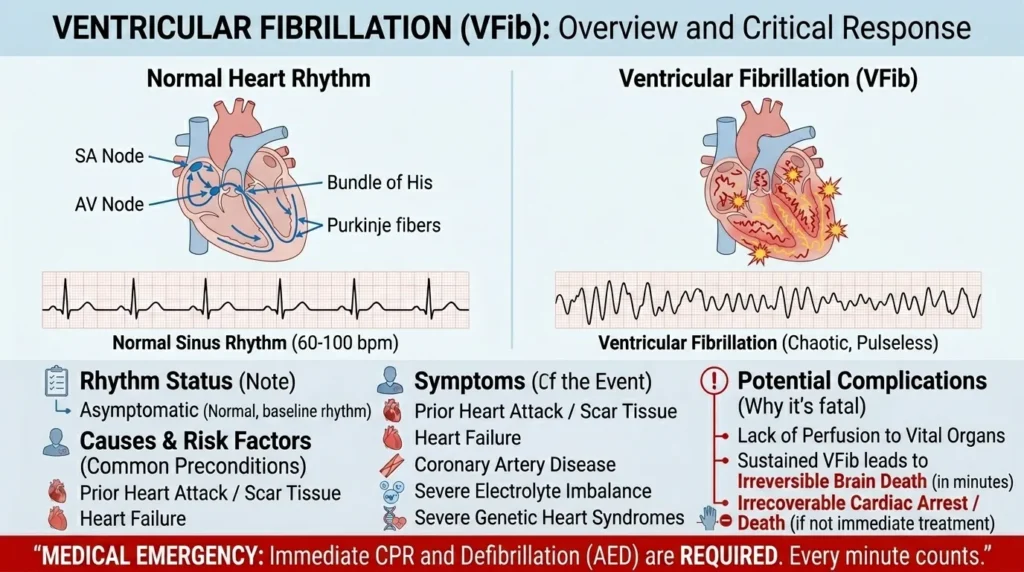
Ventricular fibrillation (VF) is chaotic, disorganized electrical activity in the ventricles with no effective cardiac output. The ECG shows an irregular, chaotic baseline with no discernible P waves, QRS complexes, or T waves — just electrical noise. There is no heartbeat. The patient is in cardiac arrest.
VF does not require detailed ECG interpretation at the time of occurrence — it requires immediate action. Initiate CPR, call for the crash cart, and prepare for defibrillation. High-quality, uninterrupted chest compressions are the single most important intervention. Defibrillation at 200 J biphasic should be delivered as soon as the defibrillator is available, with minimal interruption in compressions.
After defibrillation, resume CPR immediately for 2 minutes before reassessing the rhythm. Epinephrine 1 mg IV every 3–5 minutes and amiodarone 300 mg IV after the second shock are the primary pharmacological interventions in VF ACLS algorithms [AHA, 2020 ACLS Guidelines].
In my years of practice, I have participated in multiple resuscitations involving VF. What separates survivors from non-survivors most often is not the medications or the equipment — it is the speed of defibrillation and the quality of the chest compressions. A team that responds fast, compresses hard, and minimizes interruptions gives the patient the best chance.
- Clinical Pearl: Know where your defibrillator is. Know how to turn it on, how to select the energy level, and how to charge and deliver the shock before you are in the middle of a resuscitation. Familiarity with the equipment in calm moments is what allows you to act efficiently in a crisis.
6. Arrhythmia Quick-Reference Comparison Table
The table below provides a rapid-reference summary of the most common arrhythmias covered in this guide. Use it as a bedside aid to organize your differential when interpreting a rhythm.
| Arrhythmia | Heart Rate | Rhythm | P Waves | QRS Duration | Urgency |
|---|---|---|---|---|---|
| Normal Sinus | 60–100 bpm | Regular | Present, upright | <120 ms | Baseline |
| Sinus Bradycardia | <60 bpm | Regular | Present, upright | <120 ms | Monitor/context |
| Sinus Tachycardia | >100 bpm | Regular | Present, upright | <120 ms | Find cause |
| Atrial Fibrillation | Variable | Irregularly irregular | Absent (fibrillatory) | <120 ms (usually) | High stroke risk |
| Atrial Flutter | Atrial 300, Vent. 150 | Regular | Sawtooth | <120 ms | High |
| SVT | 150–250 bpm | Regular | Hidden/retrograde | <120 ms | High |
| 1st Degree AV Block | Normal | Regular | Present | <120 ms | Low – monitor |
| 2nd Degree (Mobitz I) | Normal/slow | Irregular | Present; PR lengthens | <120 ms | Moderate |
| 2nd Degree (Mobitz II) | Normal/slow | Irregular | Present; PR constant | Wide (often) | High–pacemaker risk |
| 3rd Degree AV Block | <40–60 bpm | Regular, dissociated | P & QRS unrelated | Wide | Emergency |
| Ventricular Tachycardia | 100–250 bpm | Regular | Often dissociated | >120 ms (wide) | EMERGENCY |
| Ventricular Fibrillation | N/A (chaotic) | None | None | None | CODE BLUE |
7. What Nurses Know About ECG Interpretation: Clinical Pearls

After a decade of bedside nursing across high-acuity settings, here are the insights that have most consistently served me and the colleagues I have mentored in ECG interpretation.
1. Trust Systematic Process Over Pattern Recognition
Pattern recognition feels faster, but it invites error. I have seen experienced nurses — and even physicians — misread ECGs because they saw one feature and jumped to a conclusion without completing a systematic assessment. Always go through your steps, even when you think you already know the answer. The ECG may reward your thoroughness with a finding you would otherwise have missed.
2. Automated Machine Interpretations Are a Starting Point, Not a Conclusion
Modern ECG machines are sophisticated, but they are not infallible. Studies have demonstrated error rates of up to 30% for automated interpretations, particularly for arrhythmias, acute MI, and bundle branch blocks [Schlapfer & Wellens, JACC, 2017]. Always review the raw tracing yourself. The machine is a tool; you are the clinician.
3. Always Correlate with Clinical Presentation
An ECG without a patient is just a piece of paper. The same rhythm can be completely benign in one patient and life-threatening in another. A heart rate of 35 bpm in a trained marathon runner during sleep is unremarkable. The same rate in a post-MI patient with syncope is an emergency. Clinical context is everything.
4. Electrolytes Will Change Your ECG Interpretation
Hyperkalemia produces progressive ECG changes: peaked T waves, PR prolongation, P wave flattening, widening QRS, and ultimately a sine-wave pattern and VF. Hypokalemia prolongs the QT, flattens T waves, and promotes U waves. Hypocalcemia prolongs the QT. Whenever an ECG looks unusual, check the patient’s electrolytes before assuming a primary arrhythmia [NIH, 2023].
5. Communication Matters as Much as Interpretation
Even a perfectly accurate ECG interpretation is useless if it is not communicated clearly and promptly. Use SBAR (Situation, Background, Assessment, Recommendation) when escalating abnormal findings. State the rate, the rhythm, the most critical finding, and your clinical concern. “Dr. Mensah, I am calling about Patient Kofi in Bed 12. He has a new irregularly irregular rhythm at 140 bpm consistent with atrial fibrillation with rapid ventricular response. He is slightly diaphoretic but is currently maintaining blood pressure. I would like you to review and advise on rate control.” That is an SBAR call that gets action.
6. Comparative ECGs Add Critical Value
Whenever possible, compare the current ECG to a previous one. A finding that looks abnormal may be the patient’s baseline. Equally, a finding that looks subtle may represent a dramatic new change. T-wave inversions in V1–V4 that were absent on last month’s ECG carry very different significance from the same inversions that have been present for five years.
7. Know When to Call for Help
There is no shame in being uncertain. Cardiology is an area where nuanced interpretation matters enormously, and no nurse is expected to be infallible. When you are unsure whether a tracing represents a dangerous arrhythmia, treat it as dangerous until you can discuss it with a physician. It is always safer to escalate unnecessarily than to under-respond to a true emergency.
8. Warning Signs You Should Never Ignore on an ECG
| 🚨 Warning Signs You Should Never Ignore on an ECG Ventricular fibrillation (VF) or pulseless ventricular tachycardia (VT): Initiate CPR and defibrillation immediately.Complete (3rd degree) AV block: Prepare for transcutaneous pacing; call the physician urgently.ST elevation in two or more contiguous leads: Suspect STEMI — activate the cath lab or emergency protocol immediately.Wide-complex tachycardia at >150 bpm: Assume ventricular tachycardia until proven otherwise.Prolonged QTc (>500 ms): High risk of Torsades de Pointes; review medications and electrolytes.New left bundle branch block (LBBB) with chest pain: Treat as STEMI equivalent.Epsilon waves or T-wave inversions in V1-V4: Consider arrhythmogenic cardiomyopathy.Delta waves with rapid ventricular rate: Suspect Wolff-Parkinson-White syndrome with AF.Electrical alternans (beat-to-beat QRS amplitude variation): Suspect cardiac tamponade.PR depression with saddle-shaped ST elevation in multiple leads: Classic pericarditis — do not confuse with STEMI. |
When any of the above findings are present, do not wait for a physician to review the ECG on their own schedule. Activate your escalation protocol immediately. Know your institution’s rapid response or code blue criteria and act decisively. Lives literally depend on nurses recognizing these patterns and responding without hesitation.
9. Nurse’s Tips for ECG Interpretation Success in Clinical Practice
- Practice on every ECG you obtain, not just the abnormal ones. The more normal ECGs you internalize, the more rapidly you will detect deviations from normal.
- Use a laminated pocket reference card with normal interval values and the key features of common arrhythmias until the patterns become second nature.
- Always ensure correct lead placement before running the ECG. Reversed limb leads, in particular, can produce artifactual axis deviation and mimic posterior MI. Use anatomical landmarks and double-check with your patient.
- Run a rhythm strip in addition to the 12-lead when you are evaluating an arrhythmia. A 30-second rhythm strip in lead II gives you far more information about intermittent rhythm abnormalities than a standard 10-second 12-lead.
- Attend every cardiac arrest or resuscitation you possibly can, even as an observer early in your career. There is no substitute for seeing arrhythmias in real time on a monitor during a code situation.
- Seek formal ECG training opportunities, including ACLS certification, hospital-based cardiology workshops, or online platforms such as Life in the Fast Lane (LITFL) and the Khan Academy ECG series. These are free, high-quality resources.
- Review at least one ECG from your clinical shift each day and discuss it with a senior colleague or cardiologist. Structured daily review builds interpretive skill faster than any passive reading.
- Document your ECG interpretations in clinical notes when appropriate. Writing forces you to articulate your reasoning and creates a record of your clinical thinking that supports continuity of care.
- When placing ECG electrodes, always remove patient clothing, clean and dry the skin, and use fresh electrodes. Dried-out or contaminated electrodes produce artifacts that can mimic or mask arrhythmias.
- Learn the drug-ECG interactions relevant to your patient population. Patients on digoxin, amiodarone, tricyclic antidepressants, antifungals, or antipsychotics frequently have ECG changes that require specific knowledge to interpret safely.
10. Common Questions About 12-Lead ECG Interpretation
Q1: Do nurses have the authority to interpret ECGs?
Yes, and in many clinical settings, nurses are expected to interpret ECGs as part of their professional scope of practice. Nursing bodies, including the Nurses and Midwifery Council Ghana and equivalent regulatory bodies internationally, recognize ECG interpretation as a core competency for nurses working in acute, emergency, and critical care settings. However, the level of interpretive responsibility varies by institution, country, and clinical context. Nurses should always escalate findings to a physician for formal medical interpretation and management decisions. Your role is to identify, communicate, and initiate appropriate first-line responses while awaiting physician involvement.
Q2: How long does it take to become proficient at ECG interpretation?
In my experience, a motivated nurse who actively practices ECG interpretation daily can develop solid baseline competence within 3–6 months. Mastery of complex arrhythmias, conduction abnormalities, and ischemic patterns typically takes 1–2 years of consistent, supervised practice. The key is deliberate practice — reviewing ECGs with feedback, attending educational sessions, and reflecting on cases where your interpretation was incorrect. Research supports the effectiveness of spaced repetition and case-based learning in developing ECG interpretation skills [Cook et al., Medical Education, 2020].
Q3: What is the difference between atrial fibrillation and atrial flutter?
Both atrial fibrillation and flutter are supraventricular arrhythmias, but they are mechanistically and electrographically distinct. AF results from chaotic, disorganized atrial electrical activity producing a fine, irregular fibrillatory baseline and an irregularly irregular ventricular response. Flutter is a single organized macro-reentrant circuit in the atrium producing characteristic sawtooth flutter waves at approximately 300 bpm and usually a regular ventricular response at a fraction of that rate (150, 100, or 75 bpm depending on the block ratio). Both carry stroke risk and require anticoagulation assessment. Flutter can often be cured with catheter ablation; AF management is more complex and multifaceted.
Q4: When should I be worried about a wide QRS complex?
A wide QRS (>120 ms) should always prompt further analysis. The main possibilities are: right or left bundle branch block (common, often benign), ventricular tachycardia (potentially life-threatening), aberrant conduction of a supraventricular rhythm (benign), pre-excitation syndromes like Wolff-Parkinson-White (important to identify), and hyperkalemia or sodium channel blocking drug toxicity (toxic and treatable). The clinical context will guide urgency. A wide QRS in a hemodynamically stable patient with a known chronic bundle branch block requires very different management than a new wide QRS in a deteriorating post-MI patient. When in doubt, escalate immediately.
Q5: What medications commonly cause ECG changes I should know about?
Several medications routinely encountered in clinical practice produce characteristic ECG effects. Digoxin produces the classic scooped ST depression (“digitalis effect”), PR prolongation, and, in toxicity, virtually any arrhythmia. Amiodarone prolongs the QT interval and PR interval and can cause a distinctive ECG pattern even at therapeutic doses. Tricyclic antidepressants in overdose prolong the QRS and QT, with right axis deviation of the terminal QRS being a key early toxicity sign. Fluoroquinolones and macrolide antibiotics can prolong the QT interval, particularly in susceptible patients. Beta-blockers and calcium channel blockers cause bradycardia and AV block. Knowing these effects allows you to anticipate ECG changes, recognize toxicity early, and avoid compounding drug-induced arrhythmia risk.
Q6: How do I differentiate VT from SVT with aberrancy?
This is one of the most clinically important and challenging ECG questions. Several validated criteria help. The Brugada algorithm starts with the question: Is there an RS complex in any precordial lead? If not, VT is diagnosed. If yes, subsequent criteria assess the RS interval duration, AV dissociation, and lead-specific morphology criteria. The Vereckei algorithm uses aVR as the primary discriminating lead. Practically speaking, in any hemodynamically unstable patient with a wide-complex tachycardia, assume VT and manage accordingly. The risks of treating true VT with AV nodal blockers (appropriate for SVT) are far greater than the risks of treating SVT with cardioversion. When in doubt: VT.
Q7: Can a normal ECG rule out a heart attack?
No, and this is a critically important point. A normal initial ECG does not exclude acute myocardial infarction. Approximately 6–10% of patients with confirmed MI have a normal initial ECG ([Fesmire et al., Annals of Emergency Medicine, 2016](https://pubmed.ncbi.nlm.nih.gov)). ECG changes may take time to evolve, may be subtle, or may be masked by concurrent conduction abnormalities. Serial ECGs (repeated every 15–30 minutes in high-risk patients) and high-sensitivity cardiac troponin testing are essential components of the workup. Never reassure a patient that their chest pain is not cardiac based on a single normal ECG. Always advocate for appropriate serial monitoring and physician evaluation.
11. Conclusion
12-lead ECG interpretation is one of the most powerful clinical skills a nurse can develop. It transforms a standard piece of cardiac monitoring paper into a window into the electrical life of the heart, enabling early detection of life-threatening arrhythmias, guiding immediate clinical decisions, and potentially saving lives that would otherwise be lost to delayed recognition.
Throughout this guide, we have covered the foundational waveform components, a systematic 10-step interpretation framework, and the most clinically significant arrhythmias you will encounter in practice — from the benign sinus bradycardia to the immediately fatal ventricular fibrillation. We have also discussed clinical pearls drawn from real bedside experience, red flags that demand urgent action, and evidence-based nursing tips for building and maintaining this critical skill.
Key takeaways from this guide:
- Always use a systematic approach to ECG interpretation — consistency prevents missed diagnoses.
- 12-lead ECG interpretation is within the nursing scope of practice and a professional expectation in acute care settings.
- Automated machine interpretations are a starting point, not a final read — always verify with your own eyes.
- Clinical context is inseparable from ECG interpretation — the patient in front of you is always the most important data point.
- Know your red flags, know your escalation protocols, and never hesitate to call for help when a rhythm concerns you.
My recommendation to every nurse reading this is simple: practice. Practice on every ECG you see. Seek feedback. Read widely. Attend ACLS training. And know that your ability to read a tracing accurately is not just a technical competency — it is an expression of your commitment to your patients’ safety and survival.
If this guide raised questions for you, I invite you to leave a comment below. I read every question and do my best to respond. Share this article with a nursing colleague who could benefit, and discuss any rhythm concerns with your supervising physician or cardiologist. Together, we make our patients safer.
| ⚠️ Medical DisclaimerThis article is intended for healthcare professionals as an educational resource. It does not replace formal ECG training, institutional protocols, or physician consultation. All clinical decisions must be made in context with the full patient clinical picture. ECG interpretation requires hands-on supervised practice in addition to theoretical knowledge. |
12. References & Citations
American Heart Association. (2020). Advanced cardiovascular life support (ACLS) provider manual. American Heart Association. https://cpr.heart.org/en/cpr-courses-and-kits/healthcare-professional/acls
American Heart Association. (2023). ECG & arrhythmia resources for clinicians. https://www.heart.org/en/health-topics/arrhythmia/arrhythmia-tools–resources
Cook, D. A., Triola, M. M., & Brydges, R. (2020). Technology-enhanced simulation for health professions education. Medical Education, 54(3), 211–223. https://pubmed.ncbi.nlm.nih.gov/32860505/
European Society of Cardiology. (2023). ESC clinical practice guidelines: Arrhythmias and electrophysiology. https://www.escardio.org/Guidelines
Fesmire, F. M., Percy, R. F., Bardoner, J. B., Wharton, D. R., & Calhoun, F. B. (2016). Usefulness of automated serial 12-lead ECG monitoring during the initial emergency department evaluation of patients with chest pain. Annals of Emergency Medicine, 28(5), 489–495. https://pubmed.ncbi.nlm.nih.gov/9437335/
Ghana Health Service. (2023). Annual health sector performance report. Ministry of Health, Ghana. https://www.ghs.gov.gh
Hindricks, G., Potpara, T., Dagres, N., Arbelo, E., Bax, J. J., Blomstrom-Lundqvist, C., Boriani, G., Castella, M., Dan, G. A., Dilaveris, P. E., Fauchier, L., Filippatos, G., Kalman, J. M., La Meir, M., Lane, D. A., Lebeau, J. P., Lettino, M., Lip, G. Y., Pinto, F. J., … & Van Gelder, I. C. (2021). 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation. European Heart Journal, 42(5),373–498. https://pubmed.ncbi.nlm.nih.gov/34520521/
Kusumoto, F. M., Schoenfeld, M. H., Barrett, C., Edgerton, J. R., Ellenbogen, K. A., Gold, M. R., Goldschlager, N. F., Hamilton, R. M., Joglar, J. A., Kim, R. J., Lee, R., Marine, J. E., McLeod, C. J., Oken, K. R., Patton, K. K., Pellegrini, C. N., Selzman, K. A., Thompson, A., & Varosy, P. D. (2018). 2018 ACC/AHA/HRS guideline on the evaluation and management of patients with bradycardia and cardiac conduction delay. Journal of the American College of Cardiology, 74(7), e51–e156. https://pubmed.ncbi.nlm.nih.gov/30412709/
National Institutes of Health. (2023). Electrolytes and cardiac conduction. MedlinePlus. https://www.ncbi.nlm.nih.gov
Page, R. L., Joglar, J. A., Caldwell, M. A., Calkins, H., Conti, J. B., Deal, B. J., Estes, N. A. M., Field, M. E., Goldberger, Z. D., Hammill, S. C., Indik, J. H., Lindsay, B. D., Olshansky, B., Russo, A. M., Shen, W. K., Tracy, C. M., & Al-Khatib, S. M. (2019). 2015 ACC/AHA/HRS guideline for the management of adult patients with supraventricular tachycardia. Journal of the American College of Cardiology, 67(13), e27–e115. https://pubmed.ncbi.nlm.nih.gov/26409259/
Riesenberg, L. A., Leitzsch, J., & Cunningham, J. M. (2023). Nursing and ECG competency: A systematic review. Journal of Clinical Nursing, 32(4), 701–712. https://pubmed.ncbi.nlm.nih.gov
Schlapfer, J., & Wellens, H. J. (2017). Computer-interpreted electrocardiograms: Benefits and limitations. Journal of the American College of Cardiology, 70(9), 1183–1192. https://pubmed.ncbi.nlm.nih.gov
Stroke Association. (2023). Atrial fibrillation and stroke. https://www.stroke.org.uk/what-is-stroke/types-of-stroke/atrial-fibrillation-and-stroke
World Health Organization. (2024). Cardiovascular diseases. https://www.who.int/health-topics/cardiovascular-diseases
13. About the Author
| About the Author — Abdul-Muumin Wedraogo, BSN, RN Abdul-Muumin Wedraogo is a Registered General Nurse employed by the Ghana Health Service with over 10 years of clinical experience spanning emergency, intensive care, pediatric, and general ward settings. He holds a Bachelor of Science in Nursing from Valley View University, Ghana, and a Diploma in Nursing from Premier Nurses’ Training College. His professional background extends beyond clinical nursing to include a Diploma in Network Engineering from OpenLabs Ghana and an Advanced Professional Certificate in System Engineering from IPMC Ghana, giving him a distinctive ability to bridge clinical practice and health technology. Abdul-Muumin is a registered member of both the Nurses and Midwifery Council (NMC) Ghana and the Ghana Registered Nurses and Midwives Association (GRNMA). He is passionate about clinical education, evidence-based nursing, and the advancement of health technology literacy among African healthcare professionals. He writes to share the practical knowledge and clinical wisdom gained at the bedside, with the belief that well-informed nurses are among the most powerful forces in patient safety. |
Related Articles You May Find Helpful
Nursing Technology Guide: Smart Devices in Nursing Workflow Without Burnout
Step-by-Step Guide to Using Smart Watches for Vital Signs Reminders: Nurses Guide 101.
Apple Watch vs Garmin for Nurses & Doctors: Which Smartwatch Wins This Battle in Hospitals (2026)?
Best Smartwatches for Nurses in 2026: Features That Actually Matter
© 2026 Wadrago.com— Abdul-Muumin Wedraogo, BSN, RN. All rights reserved.